

Both models have questionable aspects. A Global model is challenged by the disappearance of objects beyond the visible horizon. It is claimed this is due to dipping below the curvature of the earth. However, powerful telescopes will see the ship once again. A Flat Earth model can be depicted as in A flat Earth depiction of the 24 hour cycle of night and day This appears to work for the northern Hemisphere, but falls apart when trying to explain night and day in Antarctica.
What follows are links to thoughts from the Flat Earth school , as some sort of a counter-balance and stimulus to true debate. Critical thinking food for thought. Perhaps there are other explanations or views?
Earth Curvature Calculator
by Eldøy Projects
Accurately calculate the curvature you are supposed to see on the ball Earth. Uses a cosine function, works for all distances in both kilometers and miles.
| Distance | Curvature |
|---|---|
1 km |
0.00008 km = 0.08 meters |
2 km |
0.00031 km = 0.31 meters |
5 km |
0.00196 km = 1.96 meters |
10 km |
0.00785 km = 7.85 meters |
20 km |
0.03139 km = 31.39 meters |
50 km |
0.19620 km = 196.20 meters |
100 km |
0.78479 km = 784.79 meters |
200 km |
3.13897 km = 3138.97 meters |
500 km |
19.6101 km = 19610.09 meters |
1000 km |
78.3196 km = 78319.62 meters |
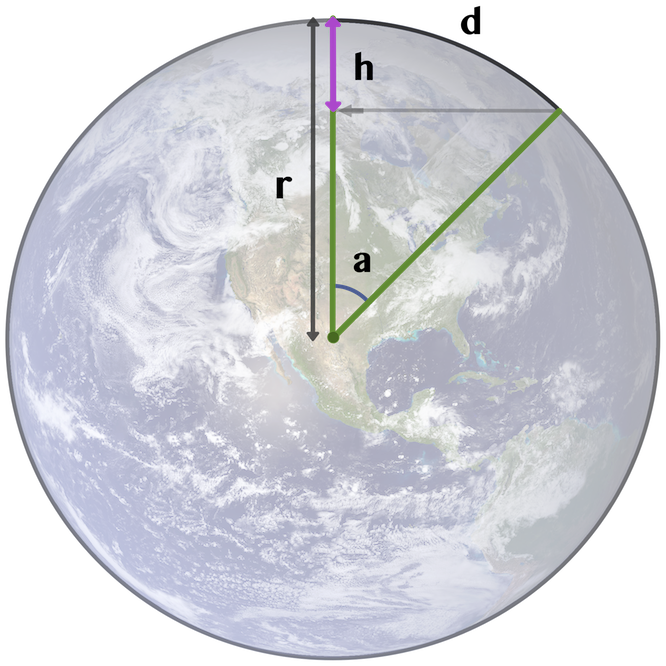
Explanation:
The Earth’s radius (r) is 6371 km or 3959 miles, based on numbers from Wikipedia,
which gives a circumference (c)of c = 2 * π * r = 40 030 km
We wish to find the height (h) which is the drop in curvature over the distance (d)
Using the circumference we find that 1 kilometer has the angle
360° / 40 030 km = 0.009°. The angle (a) is then a = 0.009° * distance (d)
The derived formula h = r * (1 - cos a) is accurate for any distance (d)
Biblical Earther
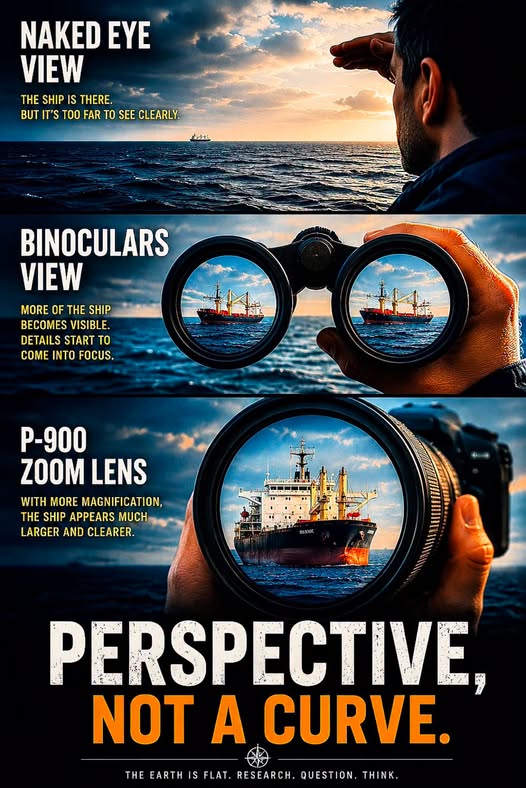
If the Earth is a ball, no amount of magnification should be able to bring a ship back from behind a wall of water. It’s not hiding behind a curve; it was just too far for the naked eye to resolve.
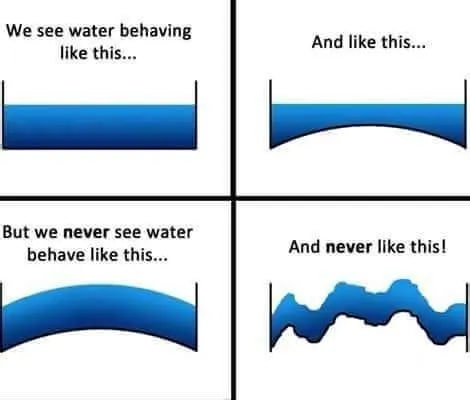
Reasons for a Flat Earth Franklin O’Kanu One of the points that really had me thinking is the concept that water always stays level. This was a thought that I really never stopped to ponder. But it’s all around us. If you look at the picture above, water always levels out. Perhaps the only exception is the meniscus which is attributed to surface tension. READ MORE https://unorthodoxy.substack.com/p/the-flat-earth-theory-a-critical
restinpeace globe
@TheGlobeIsDead
You can’t define Earth’s shape by looking into the sky. But the heliocentric model shatters under real-life observation. Check it out for yourself. https://x.com/TheGlobeIsDead/status/2060101254072688837
Does a sunset Prove we live on a Globe? https://www.youtube.com/watch?v=MZyJtgvsgdM Going Deeper: https://www.withthesun33.com/about-1
Round Earth vs. Flat Earth
Q. Why are the celestial bodies and the sun so close to the earth’s surface in the Flat Earth Model?
A. The celestial bodies must be close because if the shape of the earth changes from round to flat, the distance to the celestial bodies must change as well. Astronomers use two different observations on far off points on earth to triangulate the distance of celestial bodies. When the shape of the earth changes, the triangulation changes, and our perception of the universe must therefore change as well.
Eratosthenes’ stick experiment can not only tell us about the size of the earth, but can also be used to compute the distance to the sun as well. If the earth is round, the celestial bodies are computed to be millions of miles distant. If the earth is flat, the celestial bodies are triangulated to be relatively close to the earth’s surface.
In his experiment Eratosthenes assumes that the earth is a globe and that the sun is very far away in his computations for the size of the earth and the distance to the sun. However, if we use his data with the assumption that the earth is flat we can come up with a wildly different calculation for the distance of the sun, showing it to be close to the earth. The sun changes its distance depending on the model of the earth we assume for the experiment.
Millersville University goes over the two ways of interpreting Eratosthenes’ data. The first part of the article goes over the interpretation of his data under a Round Earth model, and the bottom part of the article goes over an interpretation of the data under a Flat Earth model.
Here’s a link which explains the idea: http://www.millersville.edu/physics/experiments/058/index.php. The first part goes over the Round Earth explanation for how the sun can be computed millions of miles distant. At the bottom there is a Flat Earth explanation for how the sun can be computed as being very close to the earth’s surface. Scroll all the way to the bottom to the “alternative model” section. You will find that we can use Eratosthenes’ data, in conjunction with the assumption of a Flat Earth, to confirm that in FET the sun is very near to the earth’s surface.
Hence, if we assume that the earth is flat and that slight travels in straight lines, triangles and trigonometry can demonstrate that the celestial bodies are fairly close to the earth.
“ Eratosthenes’ model depends on the assumption that the earth is a globe and that the sun is far away and therefore produces parallel rays of light all over the earth. If the sun is nearby, then shadows will change length even for a flat earth. A flat earth model is sketched below. The vertical stick casts shadows that grow longer as the stick moves to the left, away from the closest point to the sun. (The sun is at height h above the earth. ”

“ A little trigonometry shows that ”
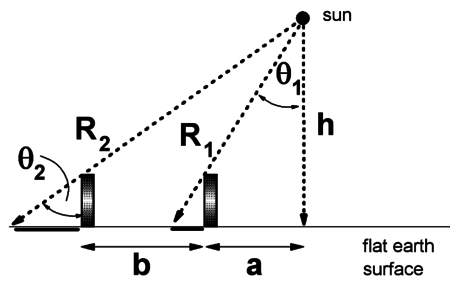
![]()
“ Using the values 50 degrees and 60 degrees as measured on the trip, with b=1000 miles, we find that h is approximately 2000 miles. This relatively close sun would have been quite plausible to the ancients.
Continuing the calculation, we find that a is approximately 2400 miles and the two distances R1 and R2 are approximately 3000 and 3900 miles, respectively. ”
There is no other way to get a distance for the sun. Just looking at it from a single point on earth will not tell you its distance, you must look at it from several points and account for the curvature or non-curvature of the distance between those points.
Please note: The writer of that article makes a unrelated side comment about the Flat Earth model —
“ That is, as we move from Florida to Pennsylvania, our distance from the sun increases by about 30%. As a consequence the apparent size of the sun should decrease by 30%. We see no noticeable change in the apparent size of the sun as we make the trip. We conclude that the flat earth/near sun model does not work. ”
This has little to do with the distance from the sun via triangulation methods. The writer of the above statement apparently did not read Chapter 10 of Earth Not a Globe. See: Magnification of the Sun at Sunset
Sun’s Distance – Zetetic Cosmogony
Thomas Winship, author of Zetetic Cosmogony, provides a calculation demonstrating that the sun can be computed to be relatively close to the earth’s surface if one assumes that the earth is flat and that light travels in straight lines —
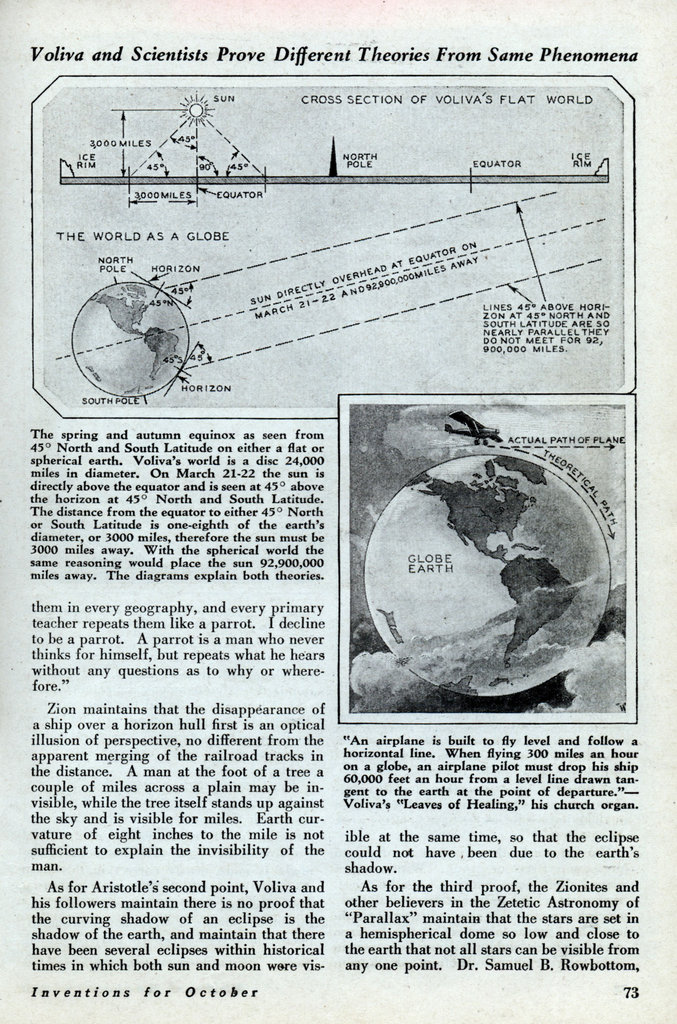
“ On March 21-22 the sun is directly overhead at the equator and appears 45 degrees above the horizon at 45 degrees north and south latitude. As the angle of sun above the earth at the equator is 90 degrees while it is 45 degrees at 45 degrees north or south latitude, it follows that the angle at the sun between the vertical from the horizon and the line from the observers at 45 degrees north and south must also be 45 degrees. The result is two right angled triangles with legs of equal length. The distance between the equator and the points at 45 degrees north or south is approximately 3,000 miles. Ergo, the sun would be an equal distance above the equator. ”
Sun’s Distance – Modern Mechanics
Modern Mechanics describes how on a Flat Earth the sun can be computed to 3,000 miles via straight line triangulation, whereas on a globe earth those same angles can calculate the sun to nearly 93 million miles away —
Distance to the Sun
The distance to the Sun and celestial bodies under the Flat Earth model varies depending on the assumptions used. Under the celestial model of Electromagnetic Acceleration where light curves, the Sun and celestial bodies can be estimated to be about 6000 miles above the surface of the Earth. Under a straight-line model, the Sun can be estimated to be about 3000 miles above the surface of the Earth.
The purpose of this page is to showcase the historic methods that have been used to determine the height of the sun and celestial bodies. Of special interest, this page will show that the Round Earth distance to the sun, and therefore the size of the solar system, relies on the idea that the earth is a sphere. The triangulation method depends on an assumption about the shape of the earth.
EA Model Estimate
If Electromagnetic Acceleration is considered, the celestial bodies are possibly about 6000 miles in altitude, which can be deduced using the North Star under the following axioms:
-
The North Star is directly over the North Pole
-
The conventional distance from the North Pole to the Equator is correct
-
The celestial bodies descend consistently in the sky with the distance you recede away from them
-
The light from the celestial bodies behave in generally the same way, and so must be in layers near to each other
From the position of the North Pole where the North Star is directly overhead, to the position of the Equator which is defined as where the North Star is seen at the horizon, the distance between the points is approximately 6000 miles according to conventional figures. Over that distance, if through EA the North Star is seen to descend or ascend in the sky consistently with consistent distance, then we know that the altitude of the North Star above the Earth is consistent with the distance between the North Pole and the equator. At the North Pole the North Star is approximately 6000 miles above the the surface of the Earth.
Brock Riddick – A flat Earth depiction of the 24 hour cycle of night and day around our world just as feasible as the global model.
🚨🌎 Stationary Earth, Local Sun Cycle ▪️ 13-Yearly Moon Cycles should equate to a 13-Month Calendar Year 📆
🌚 God’s Sky Calendar Explained—Our current Calendar is a Lie 🕰️: The Sun measures the Day, the Moon measures the Month & the Stars measure the Year. If the moon rose in the same spot every day it wouldn’t help us measure the month (Thirteen 28-day Moon Cycles should equate to a 13-month Calendar). Also, by the same logic the sun sets in a different spot everyday but always goes overhead at the exact middle of the day, every day. The stars reset to the exact same position yr after year. We live in a perfectly choreographed clock—isn’t it beautiful❗️♥️ And to further confuse us, they switched around / mis-named the Months…Oct should be 8th month, Sept the 7th, etc. All to mislead, and draw us from God and his Sky Calendar Clock❗️♥️
https://en.wikipedia.org/wiki/International_Fixed_Calendar
✅ More on our True 13-Month Calendar, while our current 12-month calendar is a Lie❗️
🌍 EXPLAINED: Level Earth Seasons, Daylight, Rotation
🌎 Firmament-Level Earth 🔥
Curiosity
@MAstronomers
🚨: Earth is not flat!!
Scientists did a 24-hour live broadcast showing the Midnight Sun in Antarctica proving that the Earth is round, because only on a sphere can sunlight behave like that.
If the Earth were flat, this effect would be impossible.
Pro-informed Choice: Does this 24 hour Antarctic video really disprove Flat Earth depiction as in the Trinity Model? If so, how ?
₿en Wehrman
@benwehrman
The 24 Hour Antarctica Sun HOAX Explained –
@EricDubay 12:20 AM · May 12, 2026
https://x.com/benwehrman/status/2053842562998231190 Remington
@MarsRevealed
What if this is the north pole?
Replying to @MarsRevealed @benwehrman and @EricDubay

A Flat Earth Map (within Antarctic Ice Wall )
石井一弘(カズ 裏コロナHP管理人&裏コロナの本 著者)
@kazu_uracorona
Translated from Japanese
I’ve come to roughly understand the mechanism of the Moon.
The Moon powers up and becomes full (all bright) as it moves away from the Sun.
The Moon powers down and becomes new (all dark) as it approaches the Sun.
Crescent moons or half-moons are the processes in between, as it powers up (brightens) or powers down (darkens).
The Moon completely disappears once every month and is reborn as a new moon.
That’s why it’s called the new moon.
The dark parts on the Moon’s surface represent a map of Earth.
The mechanism of tides is created through the ionization of seawater, reacting magnetoelectrically to produce ocean tides (the ebb and flow of tides).
The ether (number 0) was removed from the periodic table probably to hide the fact that the universe doesn’t exist, I think.
READ MORE https://x.com/kazu_uracorona/status/2045699489676267787 https://x.com/kazu_uracorona/status/2045699489676267787
Conclusion:
The Moon is not a lump of dirt, there’s no far side of the Moon, there’s no gravity or attraction on the Moon, and the Moon isn’t in space to begin with (since space itself doesn’t exist). **********
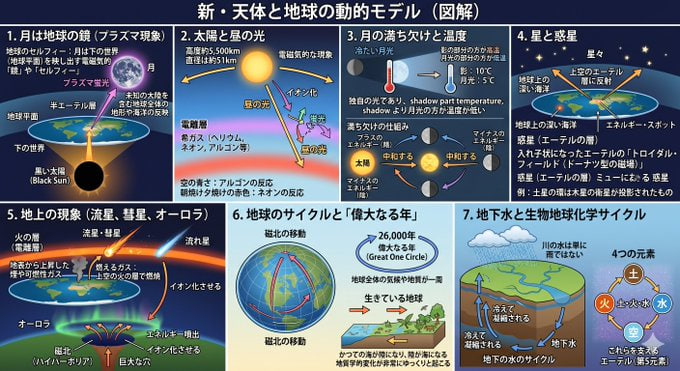
1. The Moon as Earth’s Mirror (Plasma Phenomenon)
・Earth’s Selfie: The Moon is explained not as physical land, but as an electromagnetic “mirror” or “selfie” that reflects the lower world (Earth).
・Plasma Phenomenon: Electromagnetic energy from the “Black Sun” below the flat Earth focuses in the semi-ether layer above, fluorescing to form the Moon.
・Natural Map: The patterns visible on the Moon’s surface reflect the entire geography and oceans of Earth, including unknown continents, and by looking at the Moon, one can know the true form of Earth.
2. The Sun and Daylight
・True Nature of the Sun: Like the Moon, the Sun is an electromagnetic phenomenon positioned at about 5,500 km altitude, with a diameter of about 51 km.
・Daylight (Plasma Light): As the Sun moves, rare gases in the ionosphere (helium, neon, argon, etc.) ionize and fluoresce, creating “daylight.” The blue sky is due to argon, and the red of dawn or dusk is from neon reactions.
3. The Moon’s Phases and Temperature
・Cold Moonlight: The Moon’s light is its own, not a reflection of the Sun, and experiments show that areas lit by moonlight are cooler than shadowed areas.
・Mechanism of Phases: The phases occur because the Sun’s energy (positive) neutralizes the Moon’s reflection based on their relative positions (Moon as negative energy).
4. Stars and Planets
・True Nature of Stars: Stars are reflections in the upper ether layer of deep oceans or energy spots on Earth.
・Planets (Ether Layers): Planets are projections of nested toroidal fields (doughnut-shaped magnetic fields) in the ether. For example, Saturn’s rings are explained as projections of Jupiter’s moons.
5. Ground Phenomena (Meteors, Comets, Aurora)
・Burning Gas: Meteors, comets, and shooting stars are not objects in space but phenomena where smoke or combustible gases rising from the surface burn in the upper “fire layer” (ionosphere).
・Aurora: It occurs when energy erupting from the massive hole at magnetic north (Hyperborea) ionizes the ionosphere.
6. Earth’s Cycles and the “Great Year”
・Magnetic North’s Movement: Magnetic north isn’t fixed and moves slowly. This shifts climate zones, creating a 26,000-year cycle called the “Great One Circle,” where Earth’s climate and geology complete a full rotation.
・Living Earth: Earth has cycles of growth and decline like plants or animals, with geological changes—such as former seas becoming land, and land becoming sea—occurring very slowly along with magnetic north’s movement.
7. Groundwater and Biogeochemical Cycles
・Groundwater Formation: River water isn’t just accumulated rain but is constantly newly generated by an “underground water cycle” where gases inside Earth cool and condense.
・Four Elements: Nature is composed of the interactions of the four elements “earth, fire, water, air,” supported by “ether (the fifth element).”
**********
Links:
The Flat Earth Wiki
Welcome to the Flat Earth Wiki, otherwise known as The FEW – a collaborative resource maintained by the Flat Earth Society!
This website is dedicated to unravelling the true mysteries of the universe and demonstrating that the earth is flat and that Round Earth doctrine is little more than an elaborate hoax.
The Flat Earth Society holds that there is a difference between believing and knowing. If you don’t know something, and cannot understand it by first principles, then you shouldn’t believe it. We must, at the very least, know exactly how conclusions were made about the world, and the strengths and weaknesses behind those deductions. Our society emphasizes the demonstration and explanation of knowledge.
Flat Earth Theory has grown over the centuries like a wondering sojourner hungry for truth and eager for discovery. It’s changed from the learned conjectures by our ancestors of Antiquity to Victorian polymaths like Dr. Samuel Birley Rowbotham, and it even thrives today in a world-wide grassroots effort of scholarship. This Wiki reflects these stages of Flat Earth Theory by containing information and works from each era of humanity. As people walked through the ages collecting data and knowledge, the Flat Earth Theory walked with them, growing wise and robust in kind.
We, editors of the FEW, hope that you find the truth and erudition of these works, as so many before you have. Within these digital pages you can expect to find the scepticism and understanding needed to break free from the constraints of conventional dogmatic thinking and brave the pioneering waters of true science and learning. More specifically, you will find Flat Earth proofs conducted by Flat Earthers across the world and Flat Earth concepts, terminology, and discourse. May the various Flat Earth evidence and Flat Earth maps guide your journeys to places wonderful and to ideas formerly unfathomable.
































Writes Oz’s Substack
Aug 10: