The GNM is the key to understanding the origin and behaviour of disease DR R.G.Hamer The Institute for GNM Education and Research “Introduction To The GNM” Welcome! The following video is an “Introduction To The GNM” presented by our Dean, Ilsedora Laker. Please feel free to share this resource with others as it is … Continue reading
About this Group: The German New Medicine, Applied. Insights and Perspectives from Practice discusses the science, art and philosophy of German New Medicine (Germanische Heilkunde) as developed by Ryke Geerd Hamer. Our primary focus is not geared towards teaching the basics of GNM but rather it’s application. For the past eighteen years Dr. Smookler’s singular focus has remained steadfast – the application and insights of Dr. Hamer’s most up-to-date scientific research. By joining this group you acknowledge that you understand that The German New Medicine Discussion Group is not intended for the purpose of providing medical advice. All information, content, and material of this Facebook group is for informational purposes only and are not intended to serve as a substitute for the consultation, diagnosis, and/or medical treatment of a qualified physician or healthcare provider. Please continue to follow your physician(s) medical recommendations and course of care (as I am not a medical doctor.) It’s important that you continue avail yourselves to whatever treatments, interventions and support they can provide. There are always new treatment options and I encourage you to continue to keep a close communication with your medical team. Please continue to follow your oncologists recommendations. I wish to be very clear that my protocol differs from that of my contemporaries as I will never encourage a member to abstain from or stop conventional western medical treatments
At times, it’s not simply a matter of identifying the ‘general’ or ‘gross’ conflict (macro.)
It’s often not enough for the subconscious to loosen it’s grip.
The subconscious is so precise.
If we can identify and understand the precise (micro) shadings of the priming DHS and the precise shadings of the catalyzing DHS – any and all tracks will become moot (neutralized.) The conflict is released.
When I say precise, I’m referring to the shadings, aspect, facets, flavors that need to be understood.
I am going to re-emphasize this – the vast majority of individuals that have identified the ‘general’ conflict have NOT properly identified it’s micro nuances and shadings. (There’s usually only one or two.)
These facets represent the unique ‘bits’ of the key. If we don’t find these facets we haven’t found the exacting key to unlock the subconscious.
Remember, if these shadings are imprinted on the subconscious at the moment of the DHS they need to be consciously understood, otherwise we may fall short.
One of these days I will write out my heartburn story and how although I knew what the conflict was for a long time my heartburn wasn’t budging until I was able to unearth the micro shadings tied-in with the territorial anger (despondency and resignation) which were present at the moment of the DHS.
As soon as that ‘lightbulb’ went off my heartburn lifted and has never returned.
Both models have questionable aspects. A Global model is challenged by the disappearance of objects beyond the visible horizon. It is claimed this is due to dipping below the curvature of the earth. However, powerful telescopes will see the ship once again. A Flat Earth model can be depicted as in A flat Earth depiction of the 24 hour cycle of night and day This appears to work for the northern Hemisphere, but falls apart when trying to explain night and day in Antarctica.
What follows are links to thoughts from the Flat Earth school , as some sort of a counter-balance and stimulus to true debate. Critical thinking food for thought. Perhaps there are other explanations or views?
Earth Curvature Calculator by Eldøy Projects Accurately calculate the curvature you are supposed to see on the ball Earth. Uses a cosine function, works for all distances in both kilometers and miles.
Distance
Curvature
1 km
0.00008 km = 0.08 meters
2 km
0.00031 km = 0.31 meters
5 km
0.00196 km = 1.96 meters
10 km
0.00785 km = 7.85 meters
20 km
0.03139 km = 31.39 meters
50 km
0.19620 km = 196.20 meters
100 km
0.78479 km = 784.79 meters
200 km
3.13897 km = 3138.97 meters
500 km
19.6101 km = 19610.09 meters
1000 km
78.3196 km = 78319.62 meters
Explanation:
The Earth’s radius (r) is 6371 km or 3959 miles, based on numbers from Wikipedia, which gives a circumference (c)of c = 2 * π * r = 40 030 km
We wish to find the height (h) which is the drop in curvature over the distance (d)
Using the circumference we find that 1 kilometer has the angle 360° / 40 030 km = 0.009°. The angle (a) is then a = 0.009° * distance (d)
The derived formula h = r * (1 - cos a) is accurate for any distance (d)
How far can we actually see?
Determining how far the eye can actually see is a process with many variables.
The ability to see into the distance depends on the following factors:
Visual acuity
Visual acuity is how clearly you can see things from varying distances. Perfect visual acuity is commonly known as 20/20 vision. It means you can see at 20 feet what most people with “normal” vision should be able to see at that distance.
The curve of the Earth
Global opinion:
The Earth’s roundness actually limits your view. If you’re standing at ground level with nothing in your way, the farthest you can see is to the horizon, which measures about 3 miles, or 4.8 kilometres, away.
Beyond that, the Earth gently curves out of our range of view.
Flat Earth opinion:
Human vision is limited by perspective which limits our vision to sight to around 5 km. The horizon isn’t curving away. Our vision is limited by the conversion of sight to a point called ‘the horizon’. With the aid of a telescopic lens or P1000 Nikon camera we can see much further across an earth plane or a body of water.
Reasons for a Flat Earth Franklin O’Kanu One of the points that really had me thinking is the concept that water always stays level. This was a thought that I really never stopped to ponder. But it’s all around us. If you look at the picture above, water always levels out. Perhaps the only exception is the meniscus which is attributed to surface tension. READ MORE https://unorthodoxy.substack.com/p/the-flat-earth-theory-a-critical
Q. Why are the celestial bodies and the sun so close to the earth’s surface in the Flat Earth Model?
A. The celestial bodies must be close because if the shape of the earth changes from round to flat, the distance to the celestial bodies must change as well. Astronomers use two different observations on far off points on earth to triangulate the distance of celestial bodies. When the shape of the earth changes, the triangulation changes, and our perception of the universe must therefore change as well.
Eratosthenes’ stick experiment can not only tell us about the size of the earth, but can also be used to compute the distance to the sun as well. If the earth is round, the celestial bodies are computed to be millions of miles distant. If the earth is flat, the celestial bodies are triangulated to be relatively close to the earth’s surface.
In his experiment Eratosthenes assumes that the earth is a globe and that the sun is very far away in his computations for the size of the earth and the distance to the sun. However, if we use his data with the assumption that the earth is flat we can come up with a wildly different calculation for the distance of the sun, showing it to be close to the earth. The sun changes its distance depending on the model of the earth we assume for the experiment.
Millersville University goes over the two ways of interpreting Eratosthenes’ data. The first part of the article goes over the interpretation of his data under a Round Earth model, and the bottom part of the article goes over an interpretation of the data under a Flat Earth model.
Here’s a link which explains the idea: http://www.millersville.edu/physics/experiments/058/index.php. The first part goes over the Round Earth explanation for how the sun can be computed millions of miles distant. At the bottom there is a Flat Earth explanation for how the sun can be computed as being very close to the earth’s surface. Scroll all the way to the bottom to the “alternative model” section. You will find that we can use Eratosthenes’ data, in conjunction with the assumption of a Flat Earth, to confirm that in FET the sun is very near to the earth’s surface.
Hence, if we assume that the earth is flat and that slight travels in straight lines, triangles and trigonometry can demonstrate that the celestial bodies are fairly close to the earth.
“ Eratosthenes’ model depends on the assumption that the earth is a globe and that the sun is far away and therefore produces parallel rays of light all over the earth. If the sun is nearby, then shadows will change length even for a flat earth. A flat earth model is sketched below. The vertical stick casts shadows that grow longer as the stick moves to the left, away from the closest point to the sun. (The sun is at height h above the earth. ”
“ A little trigonometry shows that ”
“ Using the values 50 degrees and 60 degrees as measured on the trip, with b=1000 miles, we find that h is approximately 2000 miles. This relatively close sun would have been quite plausible to the ancients.
Continuing the calculation, we find that a is approximately 2400 miles and the two distances R1 and R2 are approximately 3000 and 3900 miles, respectively. ”
There is no other way to get a distance for the sun. Just looking at it from a single point on earth will not tell you its distance, you must look at it from several points and account for the curvature or non-curvature of the distance between those points.
Please note: The writer of that article makes a unrelated side comment about the Flat Earth model —
“ That is, as we move from Florida to Pennsylvania, our distance from the sun increases by about 30%. As a consequence the apparent size of the sun should decrease by 30%. We see no noticeable change in the apparent size of the sun as we make the trip. We conclude that the flat earth/near sun model does not work. ”
This has little to do with the distance from the sun via triangulation methods. The writer of the above statement apparently did not read Chapter 10 of Earth Not a Globe. See:Magnification of the Sun at Sunset
Sun’s Distance – Zetetic Cosmogony
Thomas Winship, author of Zetetic Cosmogony, provides a calculation demonstrating that the sun can be computed to be relatively close to the earth’s surface if one assumes that the earth is flat and that light travels in straight lines —
“ On March 21-22 the sun is directly overhead at the equator and appears 45 degrees above the horizon at 45 degrees north and south latitude. As the angle of sun above the earth at the equator is 90 degrees while it is 45 degrees at 45 degrees north or south latitude, it follows that the angle at the sun between the vertical from the horizon and the line from the observers at 45 degrees north and south must also be 45 degrees. The result is two right angled triangles with legs of equal length. The distance between the equator and the points at 45 degrees north or south is approximately 3,000 miles. Ergo, the sun would be an equal distance above the equator. ”
Sun’s Distance – Modern Mechanics
Modern Mechanics describes how on a Flat Earth the sun can be computed to 3,000 miles via straight line triangulation, whereas on a globe earth those same angles can calculate the sun to nearly 93 million miles away —
The distance to the Sun and celestial bodies under the Flat Earth model varies depending on the assumptions used. Under the celestial model of Electromagnetic Acceleration where light curves, the Sun and celestial bodies can be estimated to be about 6000 miles above the surface of the Earth. Under a straight-line model, the Sun can be estimated to be about 3000 miles above the surface of the Earth.
The purpose of this page is to showcase the historic methods that have been used to determine the height of the sun and celestial bodies. Of special interest, this page will show that the Round Earth distance to the sun, and therefore the size of the solar system, relies on the idea that the earth is a sphere. The triangulation method depends on an assumption about the shape of the earth.
If Electromagnetic Acceleration is considered, the celestial bodies are possibly about 6000 miles in altitude, which can be deduced using the North Star under the following axioms:
The North Star is directly over the North Pole
The conventional distance from the North Pole to the Equator is correct
The celestial bodies descend consistently in the sky with the distance you recede away from them
The light from the celestial bodies behave in generally the same way, and so must be in layers near to each other
From the position of the North Pole where the North Star is directly overhead, to the position of the Equator which is defined as where the North Star is seen at the horizon, the distance between the points is approximately 6000 miles according to conventional figures. Over that distance, if through EA the North Star is seen to descend or ascend in the sky consistently with consistent distance, then we know that the altitude of the North Star above the Earth is consistent with the distance between the North Pole and the equator. At the North Pole the North Star is approximately 6000 miles above the the surface of the Earth.
🚨🌎 Stationary Earth, Local Sun Cycle ▪️ 13-Yearly Moon Cycles should equate to a 13-Month Calendar Year 📆
🌚 God’s Sky Calendar Explained—Our current Calendar is a Lie 🕰️: The Sun measures the Day, the Moon measures the Month & the Stars measure the Year. If the moon rose in the same spot every day it wouldn’t help us measure the month (Thirteen 28-day Moon Cycles should equate to a 13-month Calendar). Also, by the same logic the sun sets in a different spot everyday but always goes overhead at the exact middle of the day, every day. The stars reset to the exact same position yr after year. We live in a perfectly choreographed clock—isn’t it beautiful❗️♥️ And to further confuse us, they switched around / mis-named the Months…Oct should be 8th month, Sept the 7th, etc. All to mislead, and draw us from God and his Sky Calendar Clock❗️♥️ https://en.wikipedia.org/wiki/International_Fixed_Calendar
Scientists did a 24-hour live broadcast showing the Midnight Sun in Antarctica proving that the Earth is round, because only on a sphere can sunlight behave like that.
If the Earth were flat, this effect would be impossible.
Pro-informed Choice: Does this 24 hour Antarctic video really disprove Flat Earth depiction as in the Trinity Model? If so, how ?
₿en Wehrman @benwehrman
The 24 Hour Antarctica Sun HOAX Explained – @EricDubay12:20 AM · May 12, 2026 https://x.com/benwehrman/status/2053842562998231190 Remington
@MarsRevealed
What if this is the north pole?
Replying to @MarsRevealed @benwehrman and @EricDubay
A Flat Earth Map (within Antarctic Ice Wall )
石井一弘(カズ 裏コロナHP管理人&裏コロナの本 著者) @kazu_uracorona
Translated from Japanese I’ve come to roughly understand the mechanism of the Moon.
The Moon powers up and becomes full (all bright) as it moves away from the Sun.
The Moon powers down and becomes new (all dark) as it approaches the Sun.
Crescent moons or half-moons are the processes in between, as it powers up (brightens) or powers down (darkens).
The Moon completely disappears once every month and is reborn as a new moon. That’s why it’s called the new moon.
The dark parts on the Moon’s surface represent a map of Earth.
The mechanism of tides is created through the ionization of seawater, reacting magnetoelectrically to produce ocean tides (the ebb and flow of tides).
The ether (number 0) was removed from the periodic table probably to hide the fact that the universe doesn’t exist, I think.
Conclusion: The Moon is not a lump of dirt, there’s no far side of the Moon, there’s no gravity or attraction on the Moon, and the Moon isn’t in space to begin with (since space itself doesn’t exist). **********
1. The Moon as Earth’s Mirror (Plasma Phenomenon) ・Earth’s Selfie: The Moon is explained not as physical land, but as an electromagnetic “mirror” or “selfie” that reflects the lower world (Earth). ・Plasma Phenomenon: Electromagnetic energy from the “Black Sun” below the flat Earth focuses in the semi-ether layer above, fluorescing to form the Moon. ・Natural Map: The patterns visible on the Moon’s surface reflect the entire geography and oceans of Earth, including unknown continents, and by looking at the Moon, one can know the true form of Earth.
2. The Sun and Daylight ・True Nature of the Sun: Like the Moon, the Sun is an electromagnetic phenomenon positioned at about 5,500 km altitude, with a diameter of about 51 km. ・Daylight (Plasma Light): As the Sun moves, rare gases in the ionosphere (helium, neon, argon, etc.) ionize and fluoresce, creating “daylight.” The blue sky is due to argon, and the red of dawn or dusk is from neon reactions.
3. The Moon’s Phases and Temperature ・Cold Moonlight: The Moon’s light is its own, not a reflection of the Sun, and experiments show that areas lit by moonlight are cooler than shadowed areas. ・Mechanism of Phases: The phases occur because the Sun’s energy (positive) neutralizes the Moon’s reflection based on their relative positions (Moon as negative energy).
4. Stars and Planets ・True Nature of Stars: Stars are reflections in the upper ether layer of deep oceans or energy spots on Earth. ・Planets (Ether Layers): Planets are projections of nested toroidal fields (doughnut-shaped magnetic fields) in the ether. For example, Saturn’s rings are explained as projections of Jupiter’s moons.
5. Ground Phenomena (Meteors, Comets, Aurora) ・Burning Gas: Meteors, comets, and shooting stars are not objects in space but phenomena where smoke or combustible gases rising from the surface burn in the upper “fire layer” (ionosphere). ・Aurora: It occurs when energy erupting from the massive hole at magnetic north (Hyperborea) ionizes the ionosphere.
6. Earth’s Cycles and the “Great Year” ・Magnetic North’s Movement: Magnetic north isn’t fixed and moves slowly. This shifts climate zones, creating a 26,000-year cycle called the “Great One Circle,” where Earth’s climate and geology complete a full rotation. ・Living Earth: Earth has cycles of growth and decline like plants or animals, with geological changes—such as former seas becoming land, and land becoming sea—occurring very slowly along with magnetic north’s movement.
7. Groundwater and Biogeochemical Cycles ・Groundwater Formation: River water isn’t just accumulated rain but is constantly newly generated by an “underground water cycle” where gases inside Earth cool and condense. ・Four Elements: Nature is composed of the interactions of the four elements “earth, fire, water, air,” supported by “ether (the fifth element).”
Welcome to the Flat Earth Wiki, otherwise known as The FEW – a collaborative resource maintained by the Flat Earth Society!
This website is dedicated to unravelling the true mysteries of the universe and demonstrating that the earth is flat and that Round Earth doctrine is little more than an elaborate hoax.
The Flat Earth Society holds that there is a difference between believing and knowing. If you don’t know something, and cannot understand it by first principles, then you shouldn’t believe it. We must, at the very least, know exactly how conclusions were made about the world, and the strengths and weaknesses behind those deductions. Our society emphasizes the demonstration and explanation of knowledge.
Flat Earth Theory has grown over the centuries like a wondering sojourner hungry for truth and eager for discovery. It’s changed from the learned conjectures by our ancestors of Antiquity to Victorian polymaths like Dr. Samuel Birley Rowbotham, and it even thrives today in a world-wide grassroots effort of scholarship. This Wiki reflects these stages of Flat Earth Theory by containing information and works from each era of humanity. As people walked through the ages collecting data and knowledge, the Flat Earth Theory walked with them, growing wise and robust in kind.
We, editors of the FEW, hope that you find the truth and erudition of these works, as so many before you have. Within these digital pages you can expect to find the scepticism and understanding needed to break free from the constraints of conventional dogmatic thinking and brave the pioneering waters of true science and learning. More specifically, you will find Flat Earth proofs conducted by Flat Earthers across the world and Flat Earth concepts, terminology, and discourse. May the various Flat Earth evidence and Flat Earth maps guide your journeys to places wonderful and to ideas formerly unfathomable.
The most striking feature was the protection purported by citrus peel consumption (OR = 0.66, 95% CI = 0.45-0.95). Moreover, there was a dose-response relationship between higher citrus peel in the diet and degree of risk lowering. This is the first study to explore the relationship between citrus peel consumption and human cancers. Our results show that peel consumption, the major source of dietary d-limonene, is not uncommon and may have a potential protective effect in relation to skin SCC. Further studies with large sample sizes are needed to more completely evaluate the interrelationships between peel intake, bioavailability of d-limonene, and other lifestyle factors.
Adjusting for brewing time, the association between skin SCC and hot black tea consumption suggests a significantly lower risk in consumers of hot tea compared to nonconsumers (OR, 0.33; 95% CI, 0.12-0.87). Our results show that tea concentration (strength), brewing time, and beverage temperature have major influences on the potential protective effects of hot black tea in relation to skin SCC. Further studies with increased sample sizes are needed to evaluate the interrelationships between preparation techniques, tea type, and other life-style factors.
Have you studied the biological language your body speaks?…
Often people come across GHK and they straddle between paradigms.
They fear abandoning their yearly scan rituals.
They ask “well should I get a blood test/PAP/colonoscopy/mammogram”?
That depends entirely on YOU and your belief system.
Does it make sense to you to get it?
What information are you wanting?
What will you do with that information when you get it?
How will you respond if the result is “concerning” in the eyes of the medical system?
This is the yet another reason to learn the map of the 𝟱 𝗕𝗶𝗼𝗹𝗼𝗴𝗶𝗰𝗮𝗹 𝗟𝗮𝘄𝘀!
When you personally understand what your symptoms and lab markers indicate about what is happening you can drastically reduce the chances you’ll experience a diagnosis shock.
When you understand the source of the tissue changes and the connection to the unresolved conflict in your life you are less likely to be surprised or scared by test results….
And, most importantly, you’ll know what to do in your life to start downgrading or resolving your conflict.
Come study and explore this paradigm with me three times a month!
Comment GHK for the link to my new study + group coaching program.
Welcome! The following video is an “Introduction To The GNM” presented by our Dean, Ilsedora Laker. Please feel free to share this resource with others as it is a solid overview of Dr. Hamer’s findings explaining the 5 Biological Laws.
1. John, to begin, could you please tell us about your background and how you became involved with Dr. Ryke Geerd Hamer’s work
In 1997, I read a book that outlined Dr. Hamer’s1 discoveries. This was the first time I learned something about medicine and biology that I could actually understand, rather than just having to believe in. After reading Dr. Hamer’s books in 1997, I attended my first lecture by Helmut Pilhar in Vienna. Since then, the GHK has played a significant role in my life.
2. What initially drew you to the German New Medicine, and how has it changed your perspective on health and healing?
That I didn’t have to trust and believe in what Dr. Hamer was saying because Germanische Heilkunde is logical – it is bio-logical. There are no contradictions nor dogmas in GHK, and everyone can experience the GHK in their daily lives, in their own body.
3. Can you explain in simple terms what the “Five Biological Laws” are and why they’re considered revolutionary in understanding disease?
Every organ, every tissue, and every cell in our body has its specific task and function. If a (DHS2), a biological conflict shock arises in this task, our brain activates a special biological program (SBS3) that effectively helps us to resolve this conflict. Depending on which germ layer this tissue belongs to, the conflict results in either cell growth, cell degradation, or loss of function. This cell change, changes or improves the organ function in such a way that we can better resolve our conflict shock in real terms.
About this Group: The German New Medicine, Applied. Insights and Perspectives from Practice discusses the science, art and philosophy of German New Medicine (Germanische Heilkunde) as developed by Ryke Geerd Hamer. Our primary focus is not geared towards teaching the basics of GNM but rather it’s application. For the past eighteen years Dr. Smookler’s singular focus has remained steadfast – the application and insights of Dr. Hamer’s most up-to-date scientific research. By joining this group you acknowledge that you understand that The German New Medicine Discussion Group is not intended for the purpose of providing medical advice. All information, content, and material of this Facebook group is for informational purposes only and are not intended to serve as a substitute for the consultation, diagnosis, and/or medical treatment of a qualified physician or healthcare provider. Please continue to follow your physician(s) medical recommendations and course of care (as I am not a medical doctor.) It’s important that you continue avail yourselves to whatever treatments, interventions and support they can provide. There are always new treatment options and I encourage you to continue to keep a close communication with your medical team. Please continue to follow your oncologists recommendations. I wish to be very clear that my protocol differs from that of my contemporaries as I will never encourage a member to abstain from or stop conventional western medical treatments
Bones and Joints Understanding osteoporosis, arthritis, bone cancer, osteosarcoma, and leukemia based on the science of German New Medicine (GNM).
Cowan questions whether our symptoms and observable physical changes can be meaningfully categorized into discrete diseases, or if they instead represent individual bodies’ adaptive responses to unique life circumstances. This perspective positions disease categories as artificial constructs that subtly trap people in a victim mentality rather than empowering them with agency over their health.
Cowan invites us to consider a more individualized understanding of health – one that recognizes symptoms as intelligent adaptations rather than malfunctions requiring standardized interventions.
I recently came across Andreas Moritz, and he had me at the title of this book. Cancer Is Not a Disease – It’s a Survival Mechanism.
The conventional narrative tells us that cancer is a genetic mishap or an external viral enemy—something to be eradicated through war-like tactics. But what if that entire framework is wrong? To my mind, it most certainly is.
The body, far from malfunctioning, is trying to survive. It’s an adaptive response, a last-ditch effort by the body to manage toxicity and cellular distress. It’s not the enemy—it’s a survival mechanism. That’s a far more accurate model of reality than the one ouroligarchs and their Cartel Medicinehave sold us.
Why is the Samoan Measles narrative relevant today?
There was a supposed outbreak of measles in Samoa in September 2019.
The story provided to the World Press was that a child on holidays from New Zealand unknowingly had created an epidemic.
A ‘case’ of measles had been reported in the hospitals, which was taken to mean a spread had occurred.
This was reported to be “catastrophic” because there was a low uptake of vaccinations for Measles.
The uptake was hovering around 30% after the deaths of two babies after vaccination in 2018
Two nurses were charged with manslaughter for supposedly a mix-up in vaccine preparation.
The President had suspended the use of the vaccine for 10 months against the WHO recommendations.
The stage was set to play out a sequence for a Pandemic.
Media Hype created the fear.
Lockdowns created the political response.
Vaccines were touted as the solution.
But in reality there were about 5700 cases and 83 deaths.
The World was prepped and triggered into believing into the fear of contagion and the necessity of response.
Part of the response was the attack on those who questioned what was going on.
Edwin Tamasese, the chair of a coconut farmers’ collective,highlighted deaths in remote islands as occurring after the vaccine, thus challenging its effectiveness and safety .
The attack on Tamasese was part of an attempt to blame the death toll on mis-information from so-called ‘anti-vaxxers’.
Questions were then raised about the quality of the Indian vaccine.
At no time was RFK Jnr involved in these events.
The sequence of events coincidentally paralleled what ultimately occurred during COVID.
Conspiracy Theorists claim that the Samoan Measles ‘Outbreak’ was a trial run for all the COVID measures implemented on us only moths later.
Here is a collation of reports below from the most recent back to the early history:
The measles virus began as an imagined construct to explain why people get sick. A particle was not observed first and subsequently a virus theory was developed.
As described by a1924 article, researchers were unable to consistently observe any microbe in the bodily fluids of people with measles. Despite this, they presupposed that a minute pathogen existed that could explain sickness—what came thereafter arose to fulfil the presuppositional premise.
Some media reports suggested that if Kennedy wins the appointment forHHS secretary, outbreaks like the one in Samoa will likely occur in the U.S.
“It was a disaster and it was caused in large part by RFK Jr.,” Hawaii Gov.Josh Green told MSNBCnews anchor Jonathan Capehart. “If he becomes our lead health official, you are going to see outbreaks like this in rural communities and cities across America. Children will die or have severe disabilities.”
However, a brief look into the timeline alone of events in Samoa shows that it “absolutely does not make sense” to blame themeaslesoutbreak on Kennedy, according to Dr. Vinay Prasad, a hematologist-oncologist and professor at the University of California, San Francisco.
So let’s then turn to Samoa (and neighbouring Fiji and Tonga) in 2019. Here is the timeline
April 2019 – MMR relaunched in Samoa after a pause on the vaccination program in 2018 after two vaccine-related deaths of children. The vaccine program was poorly received by the Samoan population and uptake was low. 1st Oct 2019 – UNICEF delivered 135,000 doses of measles vaccines to Fiji, 110,500 doses of measles vaccines to Samoa (as well as supplies of vitamin A) and 12,000 doses of measles vaccines to Tonga 18th Oct 2019 – Samoa declares a measles outbreak. 24th Oct 2019 – Tonga declares a measles outbreak. 7th Nov 2019 – Fiji declares a measles outbreak (archive here) 15th Nov 2019 – State of emergency declared in Samoa after 1000 cases and 15 deaths (of which 14 were children under five)
Immediately the propaganda machine moves into action making the world believe that the problem is the fact that Samoa – for one year only – had a lower vaccination rate than the neighbouring islands…
Government of Samoa
@samoagovt
A total of 32,743 vaccinations were completed before the Mass Vaccination Campaign. Since the activation of the Campaign on 20 November 2019, the Ministry has successfully vaccinated 17,088 individuals. Free vaccinations continue to be administered for the below target groups
The MMR vaccine used in Samoa is produced by the Serum Institute of India. It has been approved and certified by the World Health Organization (WHO). It is an attenuated (weakened) live virus vaccine that is sold under the brand name Tresivac.891011
Tresivac is contraindicated for people who are allergic to eggs, gelatin and neomycin or who have had a previous life-threatening reaction to any vaccine containing measles, mumps or rubella viruses. The Serum Institute’s MMR vaccine is also contraindicated for anyone who suffers from a chronic illness such as asthma or other breathing disorder, diabetes, kidney disease, or blood cell disorders such as anemia; or from severe immune suppression caused by disease (such as cancer, HIV, or AIDS), or who is receiving certain medicines such as steroids, chemotherapy or radiation. It is also contraindicated for pregnant women.12
According to the Serum Institute, there may be a problem with giving Tresivac to people with the following conditions: thrombocytopenia purpura (easy bruising or bleeding); active tuberculosis infection; a history of seizures; a neurologic disorder or disease affecting the brain (or if this was a reaction to a previous vaccine); and a weak immune system caused by disease, bone marrow transplant, or by using certain medicines or receiving cancer treatments. The vaccine might also cause problems for anyone who has received an immune globulin or other blood product within the past year or who has received a previous MMR vaccine within the previous 28 days.12
In October 2019, a one-year-old girl died two days after being administered Tresivac at a clinic in Cuba
In 2019, the leaders of Samoa closed its borders to travelers who did not have proof of vaccination records, including its own citizens. That hardline stance against measles means that for many American Baby Boomers who contracted measles as a child and have natural, true immunity and are either living in, or traveling to, Samoa must be given a jab against an infection their immune system had already conquered. The inoculation would not be solely for measles, but would also include a faulty attenuated mumps virus.
With more than fifty measles deaths claimed by the health experts in Samoa with the current outbreak, what is sadly no longer reported are thetwo deaths from MMR that rocked the Pacific Island nation in 2018. Two babies, less than two years of age, died shortly after receiving the MMR injection, causing an uproar. The Samoa prime minister “expressed his condolences” to the families and forced the country to temporarily pull the MMR vaccine from the market.
To the gasps of those who have had children injured by the MMR vaccine, Samoan authorities did not investigate what was wrong with the vaccine. Instead, authorities focused theirprobe on two nurses, charging them with two counts of manslaughter and declaring “nothing was wrong with the vaccine.” Month’s later, astill angry motherof one of the victims demanded “answers” for the death of her child. She clearly doesn’t believe the line of propaganda being sold to her as truth.
Within Samoa, malnutrition is a “growing health concern, particularly for children.”15Vitamin A treatment costs two or three pennies per dose9 and unlike vaccines, can be administered easily by parents or other providers because it does not require special training or refrigeration. While the vitamin A shipments by citizens to reduce complications in those with measles infections are disparaged in the press and social media, UNICEF has sent 30,000 vitamin A tablets along with 110,500 doses of measles containing vaccine to the island of Samoa.16
8 December, 2019 – Samoan Government Arrests “Anti-Vaxxer” as Measles Campaign Widens Dec. 5, 2019, the Samoan government reportedly arrested a “vocal antivaccination campaigner” and charged him with “incitement” as the government widens a mass measles vaccination campaign in the small South Pacific island nation of about 200,000 people. More than 4,300 measles cases with 63 deaths have been reported since the measles outbreak began in mid-October.1
Edwin Tamasese, a Samoananti-vaccinationactivist with no medical training who was also the chair of a coconut farmers’ collective,[8] was charged with “incitement against a government order”.[44]
He had posted online comments like “Enjoy your killing spree.”[8]He encouraged people to refuse immunisation, as he believed the vaccine caused measles,[45]and even discouraged life-saving antibiotics.[8]Tamasese faced up to two years in prison.[8]
Samoan government health officials have issued a recall of the MMR (measles, mumps and rubella) vaccine after two infants, a girl and a boy, died on July 6, 2018 just hours after being given the combination vaccine at Safotu Hospital on the island of f Savai’i in Samoa. 1234
Testing is underway by the Samoan Ministry of Health to determine if the vaccines caused the deaths of the babies. Local police are conducting a separate investigation into the two cases.1234
“We’ve ceased and sent out a directive to stop and cease all vaccinations of the children with the MMR,”1 said Samoa’s Director General of Health Leausa Toleafoa Dr. Take Naseri.
TV1 in Samoa is reporting that two infants have died within minutes of receiving the measles, mumps, and rubella (MMR) vaccine.
Tala Fou brings you breaking news on the death of two young children both aged 1-year-old from the villages of Safotu and Sasina in Savaii. Both children died within minutes of being vaccinated with the MMR vacine at Safotu Hospital on Friday morning the 6th of July.
Our News Reporter Alisa Faamaoni met with both families in Savaii today. The parents of the first child Marietta and Samuelu Tuisuesue of Sasina explained in detail to Tala Fou that within three minutes of their 1-year-old daughter Lannacallystah Samuelu being injected with the MMR vaccine by a nurse she was dead. (Source.)
Clearly, the nutritional status of a country matters when it comes to lowering mortality from measles. This has certainly been the case in the United States, where measles mortality rates in the U.S. dropped by more than 90 percent during the first half of the 20th century prior to the introduction of the first measles vaccine in 1963.19
Deaths from measles had decreased from 21 deaths per 1000 reported cases during 1911-1912 to less than one death per 1000 reported cases in 1953-1962. This improved measles morality rate was owed to several factors unrelated to the measles vaccine, including better sanitation and living conditions, as well as better nutrition and improved access to health care.19
In their book, Dissolving Illusions, Bystrianyk and Dr. Humphries noted that the incidence of measles was also on a downward trend—albeit a much slower rate than the decline in mortality—before the 1963 measles vaccine. 8We know, for example, that in 1954 there were 682,720 reported cases of measles in the U.S.13 This was followed by 555,156 cases in 1955; 611,936 in 1956; 486,799 in 1957; 763,094 in 1958; 406,162 in 1959; 441,703 in 1960; 423,919 in 1961; 481,530 in 1962; and 385,156 in 1963.13
While the number of reported cases of measles went up and down from year to year, the overall trend line was downward. In fact, the trend line had been going down since 1941, when the number of reported cases totaled 894,134.13
Interestingly, in 1964 (the year after the introduction of the first killed measles vaccine), the number of reported cases of measles actually went up to 458,083.13
Bystrianyk and Dr. Humphries reasonably ask, “Was measles slowly becoming less prevalent anyway?”8
We know that measles can be sub-clinical 30 percent of the time, and the death rate had already plummeted. Like smallpox, was the disease slowly burning out? Was the rise in breastfeeding and improved nutrition contributing to fewer diagnosed cases? How many cases that were recorded as measles based on a clinical diagnosis really other viruses? Can we at all trust measles incidence statistics in the first place?8
If the trend continued as seen in the measles incidence graph, then measles incidence would have hit zero in the year 2000 without any vaccine program. Coincidentally, the year 2000 is the same year the CDC declared measles eliminated from the United States.8
A long history of measles vaccine failures For over 25 years, outbreaks have been reported in populations with vaccination rates exceeding 95 percent, undermining the mainstream assumption that vaccines are the singular solution to measles control.
Here is a documented historical record of such vaccine failures:
1985, Texas, U.S.: A study published in theNew England Journal of Medicine in 1987 analyzed a measles outbreak in Corpus Christi, Texas, where 99 percent of students were vaccinated and more than 95 percent were immune. The researchers concluded: “Outbreaks of measles can occur in secondary schools, even when more than 99 percent of the students have been vaccinated and more than 95 percent are immune.”
1985, Montana, U.S.: An article in the American Journal of Epidemiology examined an outbreak of137 measles cases in Montana, despite a 98.7 percent vaccination rate. The researchers stated: “This outbreak suggests that measles transmission may persist in some settings despite appropriate implementation of the current measles elimination strategy.”
1988, Colorado, U.S.: A measles outbreak at a Colorado collegeinfected 84 students, even though over 98 percent had documented immunity due to strict vaccination policies. Researchers concluded that “measles outbreaks can occur among highly vaccinated college populations.”
1989, Quebec, Canada: Initially blamed on low vaccine coverage, a study published in theCanadian Journal of Public Healthconcluded: “Incomplete vaccination coverage is not a valid explanation for the Quebec City measles outbreak.”
1991-1992, Rio de Janeiro, Brazil: A study published in theRevista da Sociedade Brasileira de Medicina Tropicalfound that 76.4 percent of measles cases in this outbreak had been vaccinated before their first birthday.
1992, Cape Town, South Africa: A study in theSouth African Medical Journaldocumented an outbreak where 91 percent of children were vaccinated, and vaccine efficacy was only 79 percent. The researchers concluded that primary and secondary vaccine failure contributed to the outbreak.
These are just a handful of examples from an extensive body of literature documenting measles outbreaks occurring in highly vaccinated populations — clear evidence that vaccine-induced immunity is neither lifelong nor consistently effective.
This article is about measles alone. The combination MMR shot will be discussed separately.
Highlights
A long-held notion asserts that normal childhood illnesses ultimately strengthens the immune system; could that be true?
We’ve been taught to fear illness, but should we?
Shockingly, some scientists question what measles is.
What does it mean to stop or eliminate measles? Do we really want to?
Public health officials had come to a consensus that measles was a mild disease we should live with, but then decided measles was “important” when the vaccine was licensed, for the sole reason that we now had a product to sell for it.
Sudden Infant Death Syndrome (SIDS) has become a terrifying possibility for expecting parents
Parenting protocols have changed as a result. Most parents subscribe to the Back To Sleep or Safe To Sleep Program. This virtually mandates that:
Baby must sleep on the back
All blankets, quilts need to be minimised or removed along with toys etc. to ‘avoid suffocation’
One piece ‘Onesie’s baby sleeping bags or swaddle cocoons, sleep suits are used
Monitoring devices are installed to provide constant surveillance
Many parents prefer to have the baby sleep with them on their chest or right next to them
All of these procedures are considered standard practice as the main culprits for causing SIDS are said to be apn0ea or suffocation.
VaccinationAdverseEvents are not considered to be cause or even correlation.
The downsides of the Back To Sleep Program or Safe To Sleep as it is now rebranded are:
It might reduce the incident of SIDs but it makes it almost impossible to get the child to sleep alone on their backs.
As a result the babies are given ‘contact naps’ on or with the parent.
The parent is supposed to stay awake. This limits the other daily necessary housework routines and in many cases is leading to parental sleep deprivation and exhaustion.
Many parents co-sleep with their infant for years. This is okay if everyone is a good sleeper but an enormous stress if they are not.
Unfortunately the elephant in the room is that Doctors will not discuss the possibility of increased risk of SIDS post-vaccines.
SIDS declined by half. Suffocation deaths rose by about the same amount. The death certificate cannot tell you which of those numbers is real.
What if I told you that “Sudden Infant Death Syndrome” has never described a cause of death?
SIDS is what a coroner writes when the autopsy finds nothing, the scene investigation finds nothing, and the file has to be closed anyway. It is a category defined entirely by absence — the diagnosis you reach after you’ve stopped diagnosing.
That would be a footnote, except we built policy on it.
In 1994, “Back to Sleep” launched. SIDS numbers fell by more than half over the following decade, and the campaign was declared one of the great public health victories of the century.
But Malloy and MacDorman went to the death certificates in 2005 and found something the victory lap had skipped: accidental suffocation deaths were climbing roughly as fast as SIDS was falling. A Canadian team found the same shape in 2010. By 2018 the CDC’s own data brief acknowledged it in print — SIDS down, unintentional suffocation up, “undetermined” flat.
The total number of babies who died suddenly, for reasons no one could explain, barely moved.
This infographic from The Lullaby Trust in the UK highlights common SIDS risk factors while showcasing how the ‘Back to Sleep’ campaign has been used to explain shifts in reporting trends. Although focused on the UK, it provides valuable insight into how similar narratives may have influenced SIDS classifications globally.
Cook County, Illinois, recorded 208 sudden unexpected infant deaths from 2019 to 2023. A new analysis of the deaths focused heavily on sleep environments, concluding that “unsafe” sleeping was largely to blame. But what other conditions could account for the alarming rate? And what data did the researchers ignore or exclude? Yet deeper within the report are findings that point to a much more complicated picture. Concerns about vaccines and SIDS have circulated for decades. In a2008 Age of Autism column, journalist Dan Olmsted cited a1979 internal Wyeth (now Pfizer) memorandumdescribing changes in distribution of DTP (or DTaP) vaccine lots following reports of infant deaths in Tennessee. Olmsted argued the policy appeared intended to avoid “correlations being drawn between DPT vaccine lot numbers and SIDS deaths.” Olmsted also cited “A Shot in the Dark,” a book that suggested that a cluster of infant deaths following vaccination warranted greater investigation. However,several studieshave concluded there was no evidence to support such a causal association. READ MORE
If a scientific paper offers a counter-narrative conclusion, should it be deleted from the record? Science publisher Elsevier says yes, if the topic is vaccines, because allowing doctors and parents to read it would pose a risk to public health. This raises the question: Is censorship of science really the best way to ensure public health and safety? The paper under scrutiny is a peer-reviewed analysis of three decades of vaccine adverse event reporting data which found that 75 percent of sudden infant deaths occurred within seven days of a vaccination, a statistically significant finding. Author Neil Z. Miller reviewed the medical literature linking SIDS (sudden infant death syndrome) to vaccines and proposed several pathogenic mechanisms, concluding that, “While the findings in this paper are not proof of an association between infant vaccines and infant deaths, they are highly suggestive of a causal relationship.” The main finding from the paper, titled ‘Vaccines and sudden infant death: An analysis of the VAERS database 1990–2019 and review of the medical literature,’ is represented in the below image, which was widely shared on social media since its publication in the journal Toxicology Reports, in June 2021.
This is a two-part edited version of an article published last month in DR PIERRE KORY’SSubstack. Dr Kory is an American critical care and pulmonary medicine specialist investigating the SIDS (sudden infant death syndrome)/vaccine connection. TCW published an article last month looking at the suppressed UK SIDS/vaccine connection, which you can read here.
‘THE data that sudden infant death syndrome (SIDS) is caused by vaccines has been hiding in plain sight for decades yet, unsurprisingly, our pharmaceutical-governmental public health complex has successfully suppressed it.’
I find it odd that since humans started roaming the Earth and civilisations began to flourish, producing insights and achievements one more remarkable than the other, that the Greeks, Romans, Incas, Persians, Mayans, British, Indians, Chinese (sorry if I am leaving some out), never figured out that infants should be placed on their back to go to sleep to avoid ‘strangulation in bed’.
I need to point out that most infants can sleep however the $%&! they want. From developmental guidelines: ‘Infants start rolling from their stomach to their back around 4-5 months and from their back to their stomach around 5-7 months.’
After the Back to Sleep campaign, incredibly, the post-neonatal SIDS rate dropped by an average annual rate of 8.6 per cent from 1992 through 2001.
Problem: The post-neonatal mortality rate from ‘suffocation in bed’ increased during this same period at an average annual rate of 11.2 per cent.
From 1999 through 2001, the number of US deaths attributed to ‘suffocation in bed’ and ‘unknown causes’ increased significantly. Although the post-neonatal SIDS rate continued to decline, there was no significant change in the total post-neonatal mortality rate.
Then the data really started to go sideways: from 1999 through 2015, the US SIDS rate declined 35.8 per cent while infant deaths due to accidental suffocation increased 183.8 per cent.
The data that SIDS is caused by vaccines has been hiding in plain sight for decades yet, unsurprisingly, our criminal pharmaceutical-governmental public health complex has successfully suppressed it.
In my opinion, the paper below is one of the most significant papers in the field of Pediatrics in modern times. Published in 2021, it should have been heralded as a landmark paper in public health, and its findings should have been widely disseminate
1959 marks a turning point where the UK moved from ad-hoc or local vaccination efforts to a nationally organized, NHS-supported childhood immunisation program. Just 11 years later, SIDS became a registrable cause of death. It was thought to be a ‘coincidence’ that babies suffered unexplained cot death around the time they receive their first round of vaccines. In the UK, that is currently at two, three and four months old, and there are around 200 SIDS deaths per year.
Retired research scientist Dr Viera Scheibner was one of the first to publicly make a connection. She monitored hundreds of infants post-vaccination with apnoea monitors and noticed an increased pattern of breathing irregularities. She said babies became most distressed 48 hours post vaccination, which tallies with the VAERS reports. Authorities quickly moved to discredit her, and her research was dismissed by public health bodies including the Royal College of Paediatrics and Child Health, and the WHO. In the 80s and 90s, two British doctors pushed the hypothesis that ‘abusive parents were ‘getting away with murder’…
Pennsylvania authorities brought felony charges against the parents of two different babies after police said the infants died because the parents placed them in unsafe sleeping positions, SpotlightPA reported. The deaths were ruled accidental, but police allege the parents failed to follow “Safe to Sleep” guidance, which states that babies should be put to sleep on their backs.
A Midwestern Doctor @MidwesternDoc In this powerful video Raymond Obomsawin PhD discusses all the evidence strongly linking vaccination to sudden infant death and what Dr. Archie Kalekorinos (his friend) witnessed in Australia. https://x.com/MidwesternDoc/status/1915013128724664821
Dr. Archie Kalekorinos Conversation 4 A Midwestern Doctor @MidwesternDoc
Apr 23 Here he shares that: •SIDS was strongly linked to vit. C deficiency •That infant formula did not have vit. C •Premature infants should not get vaccines unless they’d received vit C and zinc first •That he saw children die because people did not heed his advice on vaccination
Archie Kalekorinos Conversation 6 A Midwestern Doctor @MidwesternDoc
Apr 23 Here Archie discusses: •How SIDS cases often had greatly elevated D-dimer’s (e.g., well over 1000 µg/mL whereas most labs typically only measured as high as 30-40 µg/mL)
•How vitamin C could be used for cancer and treating air hunger (in lieu of morphine).
Pennsylvania authorities brought felony charges against the parents of two different babies after police said the infants died because the parents placed them in unsafe sleeping positions, SpotlightPA reported. The deaths were ruled accidental, but police allege the parents failed to follow “Safe to Sleep” guidance, which states that babies should be put to sleep on their backs.
•Since at least 1933, the medical community has known that vaccines cause infant deaths. To conceal this, those deaths were renamed “crib death” and then “Sudden Infant Death Syndrome” (SIDS), eventually being attributed to infants not sleeping on their backs.
•This revisionism is not supported by the existing evidence nor the historical changes in the frequency of SIDS. Most recently, SIDS rates have had an unprecedented decrease in tandem with the COVID-19 lockdowns reducing vaccination rates.
•The vaccine most strongly associated with SIDS, DPT, was protected for decades by the government despite knowing a large body of evidence around the world showed it killed infants—particularly when an inevitable hot lot was released. Eventually, so many injury lawsuits were filed that in 1986, the government had to give blanket immunity to the vaccine manufacturers.
•This article will concisely review the vast body of evidence showing vaccines cause SIDS and reveal the mechanism modern research has now repeatedly proven causes vaccines to trigger infant death.
An Australian groupdeveloped a way to monitor infants at home continuouslyand, like many others, was able to demonstrate non-fatal disruptions of breathing spiked following DPT and Polio vaccination (this is the most likely cause of SIDS) and that this disruption continued for over six weeks post-vaccination(hence overlapping with the typical period of death that has been observed to follow vaccination). Most importantly, the breathing often had not fully recovered by the time the next vaccine was given.1,2,3
Multiple doctors have linked the DPT vaccine to Sudden Infant Death Syndrome (SIDS), noting that SIDS peaks coincide with vaccination schedules at 2, 4, and 6 months
Since at least 1933, the medical community has known that vaccines cause infant deaths. To conceal this, those deaths were renamed “crib death” and then “Sudden Infant Death Syndrome” (SIDS), eventually being attributed to infants not sleeping on their backs
This revisionism is not supported by the existing evidence nor the historical changes in the frequency of SIDS. Most recently, SIDS rates have had an unprecedented decrease in tandem with the COVID-19 lockdowns reducing vaccination rates
The vaccine most strongly associated with SIDS, DPT, was protected for decades by the government despite knowing a large body of evidence around the world showed it killed infants — particularly when an inevitable hot lot was released. Eventually, so many injury lawsuits were filed that in 1986, the government had to give blanket immunity to the vaccine manufacturers
This article will review the body of evidence showing vaccines cause SIDS and reveal the mechanism modern research has now repeatedly proven causes vaccines to trigger infant death
Although there is considerable evidence that a subset of infants has an increased risk of sudden death after receiving vaccines, health authorities eliminated “prophylactic vaccination” as an official cause of death, so medical examiners are compelled to misclassify and conceal vaccine-related fatalities under alternate cause-of-death classifications.
Of 2605 infant deaths reported to VAERS from 1990 through 2019, 58 % clustered within 3 days post-vaccination and 78.3 % occurred within 7 days post-vaccination, confirming that infant deaths tend to occur in temporal proximity to vaccine administration. The excess of deaths during these early post-vaccination periods was statistically significant (p < 0.00001). A review of the medical literature substantiates a link between vaccines and sudden unexplained infant deaths
While the findings in this paper are not proof of an association between infant vaccines and infant deaths, they are highly suggestive of a causal relationship.
Simply delete the symptoms codes after publication…
These 261 reports produced about 1,563 symptoms that were previous on reports but now have mysteriously vanished. 53 of these 261 reports are DEATH reports, many of which are Sudden Infant Death Syndrome. The “top 30 symptoms” deleted account for 421 of 1,563 (27%).
Sudden infant death syndrome (SIDS) is the diagnosis used to define the sudden unexplained death of a child of less than one year of age.
This diagnosis is reached when the death of the infant, known as infanticide, remains unexplained after a thorough autopsy and detailed death scene investigation.
The peak incidence of SIDS occurs between 2-4 months of age.
SIDS remains the leading cause of infant mortality in Western countries, constituting half of all post-neonatal (1-12 months old) deaths.
In the following article, I will show how SIDS has been used to cover up an epidemic of infanticide in the United States. To do this, we will discuss:
The history of infant deaths since the dawn of time,
The statistically significant increase of infanticide in the 1900s,
And the campaigns used to divert attention from medical interventions
‘A recent peer-reviewed study published in the medical journal Cureus provided evidence for a positive correlation between the number of vaccine doses given to babies and infant mortality rates. The study confirmed a 2011 study conducted by the same researchers, which found a positive correlation between the greater number of vaccines given to infants in the most highly developed nations and a higher infant mortality rate.12
The initial study published in 2011 in Human and ExperimentalToxicology evaluated 2009 data from developed and under-developed nations around the world and found that the greatest number of infant deaths occurred in developed nations where infants were given the highest number of vaccine doses, totaling between 21 to 26 doses. The United States gives infants under the age of one year 26 doses of vaccines—the highest number of vaccine doses of all nations.34
Critics of the initial study claimed that the researchers did not use “the full dataset” available for all 185 nations in reaching their conclusion. In the recent study, the authors of both studies, Gary Goldman, PhD and Neil Miller, conducted several investigations to test the reliability of their earlier findings in light of the claims made by critics. They reviewed the methodology, analysis, reported results and conclusion made by their critics, as well as provided odds ratio, sensitivity and replication analysis.
Both Studies Confirm That More Vaccination is Associated With Higher Infant Mortality
Many questions about the safety of the hepatitis B vaccine have been raised by figures such as Robert Kennedy Jr., Dr. Sherri Tenpenny, Dr. Casey Means, and countless concerned parents.
But one CDC contractor, Dr. Cynthia Nevison, walked into the ACIP meeting and raised another critical question: has universal Hepatitis B vaccination, after 34 long years, even lowered Hepatitis B cases on a population level? Dr. Nevison’s answer to that question might surprise you.
And if not the vaccine, why did Hepatitis B cases plummet after 1991? Dr. Nevison addressed that question, too.
The first slide Dr. Nevison presented showed acute Hepatitis B cases over time. At first glance, it looks like universal vaccination in 1991 is the reason for the downtrend, but if you look closer, you’ll notice that acute Hepatitis B cases were already falling sharply compared to when they peaked in 1985.
I’m watching and listening to the ACIP meeting as I write and construct this article. I doubt any of those ACIP professionals have seen this next graph of VAERS identifiable deaths by days from vax date to death date:
Dr. Nevison, a CDC consultant, presented actual data on Hep B incidence, and compared it with CDC models (especially the Armstrong model) which exaggerate predicted cases (by a factor of 100 when compared with CDC’s actual numbers) if vaccine is not given to every baby.
61% of Alaskans vaccinated as children over 5 still showed antibody titers 30 years later, but only about half vaccinated at earlier ages still had antibodies 30 years later. The issue is that there is no good evidence that vaccinating very early will in fact protect through adulthood.
And sure enough, what age groups are currently developing Hep B in the US? Ages 40-60! Her analysis of CDC data also showed that the newborn vaccine program made no visible difference to the downward trend in new Hep B cases that began long before the programstarted.
What doctors fail tell you, which doesn’t make sense, is that you’re injecting a newborn baby to protect them from a disease that occurs in “drug addicts and people who have risky sex.”
The Hep B vaccine given to babies also contains FIVE TIMES the amount of aluminum deemed safe for adults
Most parents don’t realise that the Hepatitis B vaccine is given within hours of birth — for a disease that spreads primarily through adult behaviours.
⚠️ No placebo-controlled trials
⏱️ Babies monitored for just 4–5 days in studies
📉 70% of reported vaccine-related deaths occurred in children under 3
💉 Mercury and aluminium exposures
🧠 Animal studies showing neurodevelopmental harm
This isn’t about fear. It’s about facts. 📥 Visitinform-me.orgto access the full module, download the companion fact sheet, and watch expert interviews.
Author Arthur Allen observed that when the hepatitis B vaccine was recommended for infants, “resistance to vaccination began to grow from a tiny hard core of ideological opponents into a larger, more mainstream group of skeptics. … Parents who found no fault with vaccination in general could still question whether the new injections were necessary.”62
“Others felt, complacently perhaps, that they would not be raising children who would ever be putting themselves at risk of hepatitis B or that their child could get the shot later.”63
“Many Americans, it seemed, didn’t like being asked to take a risk of any kind to prevent a disease they believed they could prevent perfectly well themselves.”64
ICAN is supporting an initiative that is long overdue: suing doctors and hospitals that inject newborns with a hepatitis B vaccine without parental consent.
The hepatitis B vaccine is a case study in agency capture. The target for this product was sex workers and intravenous drug users, and the rare pregnant mother who was hepatitis B positive. The problem was that CDC could not get the sex workers and intravenous drug users to take this product. The story would have ended there if pharma didn’t stand to earn billions through a wider mandate of this product.
WHY is the Hep B shot given to every newborn in the US but not in other industrialized countries? Could it be contributing to the US having the highest first day infant mortality rate and infant mortality rate? This episode originally aired on CHD Tv
Hepatitis-B is a viral attack on the liver that is transmitted through sex, shared hypodermic needles, and iatrogenic (medical) exposure. It’s a bodily fluid transmitted virus that often occurs among those engaging in “risky behavior.”�?The Hep-B vaccination (HBV) is administered at or near birth and again between three and six months of age. It’s the beginning of a lengthy runway of hazardous pediatric vaccinations recommended by the Centers for Disease Control (CDC).
Hep-B vaccination – A Danger to Infants
If vaccines worked safely, it would be prudent to screen expectant women for hepatitis-B and exclude unnecessary Hep-B vaccinations for newborns. Maybe a Hep-B vaccination would make any sort of sense for a newborn whose mother tested positive for hepatitis-B.
Except Hep-B Vaccinations Don’t Work and They are Very Dangerous
There are examples of acute hepatitis-B among those who had been vaccinated. Those examples were from “high risk” adults, young and promiscuous, and some who were exposed to hepatitis-B in clinics and hospitals (iatrogenic exposure).
The announced removal of mercury adjuvants is a public relations distraction. Mercury based thimerosal has been replaced with aluminum hydroxide, which also creates serious adverse neurological effects.
Ironically, there is evidence of almost immediate liver damage from HBV shots. Several animal studies with low dose Hep-B vaccines have been published since the 1990s.
A recent study discovered gene mutations that led to liver cell death. This study noted that vaccine manufacturers don’t test for gene mutations in their safety tests. All the studies were reported in peer reviewed journals.
How does all this affect helpless infants undergoing the CDC’s rigorous vaccination schedule beginning at or near birth with the Hep-B vaccination?
Renowned neurosurgeon and author Dr. Russell Blaylock puts it this way: “Because the child’s brain is undergoing a period of rapid growth from the third trimester of pregnancy until age 2 years, his or her brain is at considerable risk from this insane policy” [infant vaccinations].
The statistical evidence of rapidly rising autism and SIDS (sudden infant death syndrome) is overwhelming. Yet only five percent of adverse events (at best) get reported to the adverse event reporting system (AERS), making it easier for the CDC to claim their low risk to benefit vaccine ratios.
Even with those cooked books, adverse effects and deaths from HBV vaccines greatly outnumber the hepatitis-B infections and deaths among children between 10 and 14 years of age, considered the earliest age span for hepatitis-B from “high risk behavior.”
One would get a realistic adverse event statistic by multiplying what is reported by almost ten. Most affected adversely don’t know about AERS. Others don’t want to bother with the level of effort required, while many doctors prefer to deny giving a shot that destroyed a child’s life.
The CDC has steadily increased the vaccination schedule since the late 1970s, inserting the Hep-B vaccination�?shot in the 1990s. Autism has skyrocketed by almost 90 percent in three decades. Sudden infant death syndrome (SIDS) has also jumped dramatically within the USA, which is leading industrialized nations in that category.
A number of peer-reviewed studies have also found a relationship between the hep-B vaccinations�?and infant deaths both in the U.S. and Europe. With links to sudden infant death syndrome (SIDS),multiple sclerosis, and numerous chronic autoimmune disorders, some doctors are speaking out against the dangers of the hep B vaccine.
Nevertheless, mainstream medicine overall still constantly promotes vaccine safety and efficacy for HBV shots and all others. They continually dismiss those statistics as not scientific evidence for causality; while freely using epidemiology statistics, often manipulated, for their purposes.
Don’t fall for their spin. Spare your child’s future, and yours, the agony of constant suffering and medical care from adverse vaccine injury damage. If a pregnant woman doesn’t have hepatitis-B, the Hep-B vaccination�?shouldn’t even be considered.
Vaccinations are risky at any age. Before two years, when HBV vaccinations are scheduled, negative health results are highly probable later if not sooner.
[SaneVax: Despite the fact that hepatitis B is most commonly transmitted to infants via their infected mothers, the CDC recommends a 3 dose series of hepatitis B vaccinations beginning on the first day of life. Would it not make sense to test the birth mothers to determine the infant was at risk of contracting the disease prior to deciding whether vaccination is the right choice?]
Federal Court Admits Hepatitis B Vaccine Caused Fatal Auto-Immune Disorder
By Elizabeth Renter
Hepatitis B at birth worth the cost?
In our society today, newborns are injected with loads of chemicals nearly as soon as they enter the world. In the name of “prevention”, we give them vaccines that we aren’t even sure are safe. As a matter of fact, in many cases, we know them to be unsafe. This is the case with the hepatitis B vaccine, approved for infants at birth but admittedly responsible for causing serious illness and even death.
The United States Court of Federal Claims sided with the estate of Tambra Harris, who died as a result of an auto-immune disease called systemic lupus erythematosus (SLE). The court awarded $475,000 following her death after finding the hepatitis vaccine caused her injury in the form of SLE. But this near-admittance of a cause-effect relationship between the vaccine and the illness and subsequent death isn’t enough. No, we still give the shot to babies.
So, what is hepatitis B and why are we told that it is so important that newborn infants are vaccinated against it? Hepatitis B is not pleasant and can be deadly. But newborns (and the vast majority of people at any age) aren’t at risk of contracting the disease. It’s spread by contact with bodily fluids, as in through unprotected sex or dirty needles.
The risks associated with the hepatitis B vaccine are far more pressing than the risk of contracting the disease, says Dr. Jane Orient of the Association of American Physicians and Surgeons (AAPS). “For most children, the risk of a serious vaccine reaction may be 100 times greater than the risk of hepatitis B.”
The hepatitis B vaccine triples the risk of developing multiple sclerosis
Hernán MA, Jick SS, et al. Recombinant hepatitis B vaccine and the risk of multiple sclerosis: A prospective study. Neurology 2004 Sep 14; 63(5): 838-42.
“These findings are consistent with the hypothesis that immunization with the recombinant hepatitis B vaccine is associated with an increased risk of multiple sclerosis.” – Some previous studies that evaluated a potential link between the hepatitis B vaccine and an increased risk of multiple sclerosis had significant methodological limitations. – In this study, the General Practice Research Database (GPRD), containing comprehensive medical records from clinical practice in the United Kingdom, was utilized to compare 163 patients with a confirmed diagnosis of multiple sclerosis to 1,604 randomly selected controls. – Patients with multiple sclerosis were 3 times more likely to have been vaccinated against hepatitis B within 3 years before the date of first symptoms when compared to controls who were not vaccinated (odds ratio, OR = 3.1).
Miller, Neil Z.. Miller’s Review of Critical Vaccine Studies (p. 168).
Hepatitis B Vaccination of Male Neonates and Autism Diagnosis, NHIS 1997–2002
Hepatitis B triple series vaccine and developmental disability in US children aged 1–9 years
Premature Puberty and Thimerosal-Containing Hepatitis B Vaccination: A Case-Control Study in the Vaccine Safety Datalink Recombinant hepatitis B vaccine and the risk of multiple sclerosis_ a prospective study – Abstract
A Cross-Sectional Study of the Association between Infant Hepatitis B Vaccine Exposure in Boys and the Risk of Adverse Effects as Measured by Receipt of Special Education Services Hepatitis B Vaccination of Male Neonates and Autism Diagnosis, NHIS 1997–2002
Dan Dicks, long-time investigative journalist “in” Canada, is being lauded for his “real journalism” in covering the British Columbia ostrich farm angle of the “avian influenza” virus/contagion/antibodies hoax:
In 2020, we started investigating thevirus modeland came to the realisation that SARS-CoV-2 did not exist. In fact, there was no scientific evidence that any viruses existed, dating back to the late 1800s literature and the so-calledTobacco Mosaic “Virus”. Those critiquing virology have pointed out that no entity that meets the description of a virus has ever been physically isolated. In order to maintain the illusion, the virologists have not performed properlycontrolled experiments such as those proposed in the “Settling the Virus Debate” Statement.
The narratives stemming from virology’s pseudoscience are now used to control populations in every possible way by keeping them in a state of fear. The phantom “viruses” and the invented “countermeasures” also enable vast transfers of wealth from the public to governments and their favoured friends, while allowingreal and sickening globalist agendasto roll on. It is therefore more important than ever to help more people see beyond the virus model, both for their own health and the future of humanity. While for some individuals this requires a scientific treatise such as Mark’sA Farewell to Virology, for many others they simply want to know, “if it’s not a virus, what’s making me sick then?” In this video, I answer that question with my top 40 reasons…
In mid-2024, the legendary Vera Sharav of theAlliance for Human Research Protectionsent a request. She asked if my husband Mark and I would write an essay concerning the perversion of science for her companion book to the documentary“Never Again is Now Global”.
The task for our chapter was to “unmask the viral paradigm” and bidA Farewell to Virologyin non-technical language, while still citing scientific reports.
Our essay provides the overview of how the “pandemic” was staged and in some ways is a summary of part of our latest book,The Final Pandemic.
Jerm and Dr Tom Cowan discuss the COVID pandemic, questioning virus myths and medical authority. They highlight flawed virus isolation, unreliable PCR testing, and the body’s natural healing. They explore detoxification, challenge contagion theories, and debunk myths about bacteria, rabies, and the immune system. They stress the need for a scientifically literate society to build a healthier culture.
In this episode, Alec explores the misconceptions surrounding infectious diseases and reframes how we understand sickness. He examines the role of belief in health, gaps in virus research, and alternative reasons for individual and group illness. Discover insights into biofield interactions, the intelligence of water as it relates to our body, and how shifting your perspective can unlock new paths to wellness.
What if viruses don’t exist at all? – In this explosive interview, Dr. Tom Cowan — longtime physician and author of The Contagion Myth — makes the shocking case that everything we know about viruses and germ theory is wrong. – He says illness comes from toxins, not contagion — and mainstream science doesn’t want you to hear it. – Watch now and decide for yourself: medical truth-teller or dangerous heretic?
Kim Iversen 🇺🇸 @KimIversenShow I spoke with Dr Tom Cowan who challenges the idea that viruses even exist. What he says may be controversial, but it will definitely get you thinking👇 https://x.com/KimIversenShow/status/1907086569544036726
This video, presented by Caroline Markolin, Ph.D., provides an in-depth analysis of the standard “Virus”-theory in the context of German New Medicine (GNM). More information is available athttps://learninggnm.com.
The findings of this investigation align with what is seen in the published literature. Find all of the official documents (FOIs) and emails with virologists here: https://www.bitchute.com/video/gvu4NbieSuVb/
In this dynamic interview, Christine Massey shares her groundbreaking research into the issue of whether the COVID “virus” has been proven to exist, as well as the broader question as to whether any “virus” has been proven to exist.
Christine Massey has a master’s degree in bio-statistics and has worked in cancer research.
The controversy over whether the COVID “virus” has been proven to exist, is confusing to most people, but Ms. Massey pursued a route that was purely objective in doing this research. She submitted a Freedom of Information Act (FOIA) request to 213 medical institutions in 40 different countries asking them for documents that proved that the COVID virus has been purified and proven to exist. The responses she received from these institutions were absolutely shocking and draws into question everything they have been telling the public!
By Enders’ own admission, both in his 1954 paper and in public statements, critical links in thelogical chain of causationwere absent.
In formal terms, these criteria—summarized asKoch’s Postulates—require that the suspected microorganism be consistently found in all cases of disease, isolated independently of host material in pure culture, shown to reproduce the disease when introduced into a healthy host, and then recovered from that experimentally induced illness. Enders’ own evidence makes it clear that even the first two steps (consistency in cases and isolation in pure culture) were not fully satisfied, and the final steps (disease reproduction and re-isolation) remained unperformed at the time his findings were publicly declared a discovery.
Another FOIA failure, consistent with the pseudoscientific literature
My order was for:
All studies in the possession/custody/control of the Animal and Plant Health Inspection Service, Department of Agriculture, authored by anyone, anywhere:
1. – that scientifically prove/provide evidence of the existence of any alleged “avian influenza virus” (showing that the alleged particles exist, invade and replicate in “host” cells and cause the illness/symptoms that they are alleged to cause), or
2. – that (at least) describe the purification of particles that are alleged to be “avian influenza virus” directly from bodily fluid/tissue/excrement of so-called “hosts”, with purification confirmed via EM imaging, or
3. – wherein the purported “genome” of any alleged “avian influenza virus” was found intact in the bodily fluid/tissue/excrement of a “host” (as opposed to fabricated in silico, aka a computer model), or
4. – that scientifically demonstrate contagion of the illness / symptoms that are allegedly caused by purported “avian influenza viruses”. My July 21, 2024FOIA orderfiled with the U.S. Animal and Plant Health Inspection Service, Department of Agriculture finally came to completion in March of this year. It resulted in a grand total of zero responsive records being provided or cited by the “experts” there.
The person most likely to have died from a “virus” just so happen to be Military aged Males… No these men were not dying because of the bullets and bombs, chemical agents and stuff, they were all accounted for and the ones that survived just so happened to, as soon as the war ended, get a cold, keeled over and died. The average age of normal “seasonal Flu” deaths is ~80yrs old, so by some complete random chance this “transmissible pathogen” STILL killed predominantly military aged men, despite the total number of deaths being 5 times that of deaths directly attributed to war, in absolute contradiction to every other “virus” in history.
The Rosenau Study
They took 100 hundred healthy men between the ages of 18-30 yrs old. This corresponds exactly to the claimed average age of “Spanish Flu” deaths being 28yrs old. They stipulate in the study that they believe them to be of a “susceptible” age. This is in stark contrast to every other Contagion Study ever conducted. Usually they deem the most “susceptible” ages to be too vulnerable and too risky to experiment on, given that the average age of death for all other supposed respiratory viruses is nearly 80 yrs old.
They made sure to select men who had experienced no recent respiratory infection so the rescue device of “immunity” when they inevitably fail the contagion study does not apply in this instance.
They put the fluids obtained from people said to be dying with “Spanish Flu” directly up the nostrils of these healthy volunteers. Starting with a “moderate amount” which returned negative results. Then they turned up the heat by putting a “very large quantity” of fluids contained from the lungs of deceased patients died supposedly of “Spanish Flu”.
The DAMNING evidence is in the DIRECT contagion studies carried out. The Rosenau studies in my opinion are the most devastating studies to Germ Theory ever produced. When you actually look at it they were not just studying “viruses” because it wasn’t a supposed “purified Viral Culture” they were inoculating with, these contain antibiotics which kill bacteria, parasites and fungi.
These studies showed that CONTAGION of ANY pathogen is a myth as they were taking the fluids direct from sick people and transferring them to healthy people, bacteria, parasites and all.
No one has valid scientific evidence to show that “avian influenza virus” H5N1 (or any other alleged “virus”) even exists. I challenge anyone to prove me wrong by citing such evidence.
Resources for farmers
For anyone approached by government agents who want to test for (imagined) viruses in their livestock, the Weston A. Price Foundation (WAPF) created anAction Alert formthat can be given to the agents before allowing them entry to the land. The form requires the agent(s) to identify themselves and to cite valid scientific evidence of the alleged virus in question, as well as contagion of the relevant illness and validation of the tests.
– As we delve into Alec Zeck’s 2.5-hour presentation, Reframing the Infectious Disease Paradigm* , we encounter a rigorous critique that challenges this paradigm’s foundations.
The measles virus began as an imagined construct to explain why people get sick. A particle was not observed first and subsequently a virus theory was developed.
As described by a1924 article, researchers were unable to consistently observe any microbe in the bodily fluids of people with measles. Despite this, they presupposed that a minute pathogen existed that could explain sickness—what came thereafter arose to fulfil the presuppositional premise.
The work of Cowan and others are leading the way on questioning the foundations of virology.
‘Catching colds via viruses’ was studied for 44 years by the Common Cold Unit. Remains unproven.
“Novel pathogen” that “leaked” from a lab that spread around the world killing people in 2020. Disproved by the work of Rancourt.
Can they make stuff in labs that can make people sick or dead? Sure.
Can you use that to start a “pandemic” panic, with the media doing the rest. Sure.
But can they make something from genetic matter that “can pandemic.” I am confident the answer is no. It is not biologically plausible. So in that context, the biolab risk is wildly exaggerated for financial and industrial “pandemic preparedness” reasons.
30 July, 2024 – No “Virus” has ever been isolated No “Virus” has ever been isolated. A thread Here is one of 12 experiments in over 90 cultures, all with the same results. There is NO SAMPLE in these cultures and hence NO possibility of “a Virus” yet we see here CPE (Cell death) indicative of the presence of a “virus”.
Every institution has failed to provide or cite even 1 record describing the isolation aka purification of the alleged “COVID-19 virus” directly from a patient sample that was not first adulterated with other sources of genetic material. (Those other sources are typically monkey kidney aka “Vero” cells and fetal bovine serum).
(And, to our knowledge, no one on the planet has ever purified the alleged “virus” even from a cell culture! The CDC was FOI’d and had no records.)
In their responses, numerous institutions have made it explicitly clear that isolation/purification is simply never done in virology, and that “isolation” in virology means the exact opposite of what it means in everyday English. This is also evidenced in every “virus isolation” paper we have ever seen, for any alleged “virus”.
In this video, we look at a Freedom of Information Act Request that the CDC provided that they say constitutes “proof” that Covid is a virus, is contagious and that it causes disease.
We go through source by source to show that this is inaccurate. We compare electron microscope images of “Covid” and show there are identical particles known to exist in cells already and researchers pointed this out in 2020.
We review the inappropriate controls used to compare “Covid” testing.
In this video, we continue with the discussion about antibodies, we look at the first acknowledged paper that references the idea of antibodies by Emil Von Behring and Kitashato Shibasaburu in relation to diptheria.
We briefly touch on their relationship to Robert Koch (who proposed Koch’s postulates). We then look at multiple failures of the diptheria vaccine that supposedly is conveying said antibodies to people. We then look at that fact that other entities, including vitamin C have been shown to neutralize diptheria.
So, if we haven’t isolated an antibody, and we know other things can neutralize diptheria, how can we come to conclusion that antibodies necessarily convey immunity?
In this video, we continue looking at the evidence for Antibodies going back to the time of Paul Ehrlich and explore the evidence of the “Side Chain” theory.
We briefly discuss the evidence of the effect of Vitamin C on both diptheria and tetanus to demonstrate that neutralization is not exclusive to the antibody idea.
We look at Ehrlich’s presentation to the Royal Society and some of his research works on “side chain” theory and find much of his experimental evidence is lacking.
In this video, we continue to look the supposed benefits anti bodies or the class of particles called Gamma Globulins that they supposedly constitute.
We will see that it appears there are some useful clinical applications for their use at times but we covered side effects, including potentially fatal ones, in the previous lecture.
We will touch on potential environmental exposures that could be causing symptoms expressed in agammaglobunemia which would been use of gamma globulins is indicated. We will cover electrophoresis as an isolating agent and how fragile a process this can be.
In this video, we finally discuss the origin of the supposedly “unique:” anti-bodies suchas IgG, IgM, and IgE etc., how ultracentrifugation is used to identify differences in anti bodies.
Yet we keep finding new sources of potential error but no reproducibility studies of old literature?
We see more examples of both antibodies and white blood cell counts not being sufficient to explain immunity. And finally we look at the side effect profile of administering these immunoglobulins.
This lecture is the culmination of several other lectures so reviewing the lectures on CPE, cDNA and the previous Renin, Hypertensin, and angiotensin lectures will be necessary to understand it.
We deconstruct the idea that ACE 2 is a membrane bound receptor. We will see that they did not do appropriate experiments to determine that Sars Cov 1 attached to ACE 2 and the problem compounds with Covid 19. We will see that despite multiple recommendations since 2020 to use ACE 2 blocker when we actually implement the practice there is no noticeable difference in “Covid” outcomes.
So, how can we say ACE 2 is the entry point for the virus into cells if in the real world when we use medications to block the receptor it does impact the disease at all?
In this video, we finally cover staining procedures for viewing images of virus in electron microscopes.
We review the work of Harold Hillman and his disputing of current views on electron microscope and the nature of artifacts in the slides.
We cover the staining process used on “Covid 19” that requires uranyl acetate and lead citrate, both of which have confirmed toxicity to kidney tissues which is what Covid virus images are tested against.
Dan Dicks, long-time investigative journalist “in” Canada, is being lauded for his “real journalism” in covering the British Columbia ostrich farm angle of the “avian influenza” virus/contagion/antibodies hoax: This Is Universal Ostrich Inc. – A Deep Dive With Press For Truth, featuring Dr. Andrew Kaufman and Christine Massey
Because “they” (HIV, influenza virus, HPV, measles virus, etc., etc., etc.) have never been shown to exist, clearlydon’t exist and virology isn’t a science.
The mothers of 10-year-old Isabella Zuggi and 14-year-old Sydney Figueroa filed wrongful death lawsuits against Merck, alleging the company knowingly failed to warn the public and medical providers about the risk of injury or death from its Gardasil human papillomavirus vaccine.
In part 1 and part 2 of this series, we discussed the HPV vaccine and its links to ovarian insufficiency and autoimmune disease. In part 3, we turn to questions regarding the effectiveness of the vaccine to prevent cervical cancer, and the limitations of relevant clinical trials to detect such a type of effect.
In this HPV vaccine series, Parts I and II explain how the vaccine works and the evidence suggesting there may be legitimate safety concerns. The remaining parts present questions about real-world vaccine effectiveness and identify specific ingredients which may pose harm.
Vaccination is unjustified if the vaccine carries any substantial risk, as healthy teenagers face little to no risk of dying from cervical cancer. Risk-benefit analyses must be conducted to ascertain the overall balance of benefits and harms on both individual and societal levels.
As of April 16, 2023 VAERS Reported 73,366 Adverse Event Reports 10,949 Serious Reports (about 15%)555 DeathsOnly 1% of all Adverse Events get Reported
* * * * * *
Documentaries and Videos:
“Not a Coincidence”
The CDC and FDA routinely dismiss serious injuries and deaths as “coincidences” without investigation. The young persons in this short video attest that their injuries and deaths are not a coincidence and they plead for Congressional hearings about Gardasil.
Listed here are four well researched and well presented books regarding the HPV vaccines, Gardasil and Cervarix:
1. The HPV Vaccine on Trial – Seeking Justice for a Generation Betrayed
Mary Holland , J.D., Kim Mack Rosenberg, J.D.,Eileen IorioAn Important, comprehensive and well-documented book with a preface by Nobel Prize winner, DR. LUC MONTAGNIER: “This book reveals the tragedy of the HPV vaccine scandal.”
2. Shattered Dreams – The HPV Vaccine Exposed
Christina England Documented stories of injury and death and chapters by 13 professionals including Chris Exley, PhD.D
3. Journeys from Trust to Tragedy
Norma Erickson
Dedicated to the stories of some of those who suffered HPV vaccine injuries or death
4. From Pap Smear to HPV Vaccine: The Cervical Cancer Prevention Industry
Sin Hang Lee, MD Director, Milford Molecular Diagnostics Laboratory, Milford, CT, US
This in-depth book by world renown HPV expert Dr. Sin Hang Lee provides a comprehensive analysis of how the HPV industry has invaded and eroded the women’s health care system in the field of cervical cancer prevention.
* * * * * *
Research Papers and Letters (also see the page “Links to Research on Gardasil” with 90+ studies) :
Dong Y. Undeniable Death Cases After HPV Vaccination. The HPV Vaccine: A Double-Edged Sword? (Part 1). June 25,2023. Accessed 7/27/2023 at:
Tomljenovic L, Tarsell E, Garrett J, Shaw CA, Holland MS.Significant Under-reporting of Quadravalent Human Papillomavirus Vaccine-Associated Serious Adverse Events in the United States:Time for Change? Science, Public Health Policy and the Law .Volume 2:37–58 May, 2021 Clinical and Translational Research.
Researchers found that the CDC has been failing to acknowledge and record as serious reports of citizens who suffered “persistent or significant disability/incapacity” following vaccination even though that is one of the criterion defining a Serious Adverse Event (SAE) in the Code of Federal Regulations. Many youth suffered “persistent or significant disability/incapacity” following HPV vaccination. The study explores in detail the effect the failure to use the correct criteria had on detecting safety problems for Merck’s HPV vaccine, Gardasil.
Brawer AE and Sullivan, DH. The expanding cocktail of harmful ingredients in human papillomavirus vaccines. Open Access Text.DOI: 10.15761/FWH.1000195
The study documents the presence in HPV vaccines, Gardasil and Gardasil 9, of an undisclosed, highly toxic chemical called PMSF (phenylmethylsulfonyl floride). PMSF, also known as Toluene, is a serine protease/acetylcholinesterase inhibitor. Toluene is a nerve agent which can inactivate central nervous system functions. When the enzyme acetylcholinesterase is blocked, there could be uncontrollable firing of motorsignals which can manifest as seizures or other biochemical or physiological disorders.
PMSF has been used as a nerve agent in biological warfare! PMSF is used in the manufacturing of the HPV vaccine, but is not supposed to be in the final product. This paper documents that PMSF is in the final product and could initiate the onset of a host of serious adverse events that have been reported following HPV inoculations. Such outcomes include cardiovascular events, motor neuron disorders, autoimmune disorders, cognitive and mood disorders, neurological disorders, gastrointestinal disorders, miscarriages, menstrual disorders, seizures, headaches, extreme fatigue, skin disorders, sleep disorders, paralysis, encephalitis and even sudden death. A link to the paper is here:
The European Medicines Agency (EMA) was asked to investigate the HPV vaccines due to the high number of consumers who reported serious adverse events. The EMA’s cursory investigation was highly criticized in an open letter by the Nordic Cochrane group. The researchers and doctors who signed the letter complained that the EMA’s investigation was “definitely not designed to uncover any real problems that may exist with HPV vaccines. The arbitrary and most likely pre-ordained conclusion must not go unchallenged”.
Open letter to the EMA from the Nordic Cochrane group with scathing criticism of the EMA’s superficial investigation of the hpv vaccine.
Tomljenovic L, Shaw C. Human papillomavirus (HPV) vaccine policy and evidence-based medicine: Are they at odds? Annals of Medicine, Dec. 2011.
The authors conclude that the efficacy of HPV vaccines in preventing cervical cancer has not been demonstrated….
Serious adverse reactions including deaths, convulsions, paralysis, GBS, autoimmune disorders, chronic fatigue, deep vein thrombosis, pulmonary embolisms, anaphylaxis and cervical cancer remain to be fully evaluated.
The long-term health of many women may be at risk against still unknown vaccine benefits.
Tomljenovic L, Shaw C. Death after Quadrivalent Human Papillomavirus (HPV) Vaccination : Causal or Coincidental?
Researchers found evidence ofcerebral blood vessel wall immunoreactivity with HPV-16L1 which appears to have triggered fatal vasculopathy in two cases of sudden unexplained death following Gardasil vaccination. They conclude that HPV vaccines containing HPV-16L1 antigens pose an inherent risk for triggering potentially fatal autoimmune vasculopathies. The full report is published at
January 14, 2016 Dr. Sin Hang Lee sent an open letter of complaint to the Director General of the World Health
Organization, Dr. Margaret Chan, charging members of GACVS, the CDC, the Japanese Ministry of Health, Labor and Welfare, and others with manipulation of data and suppression of science in order to maintain the illusion of HPV vaccine safety in the face of valid contradictory evidence:
independent laboratory under the direction of HPV expert, Dr. Sin Hang Lee, analyzed thirteen different lots of Gardasil collected worldwide. All vials were found to be contaminated with HPV DNA. This is significant because residual DNA in a vaccine can trigger autoimmune disease, anaphylactic shock or tumors. Merck and the FDA heretofore had denied that there was any HPV DNA in Gardasil. Dr. Lee’s research paper regarding these findings and the implications is published in the Journal of Inorganic Biochemistry:
To assess if there might be patterns to reported adverse events following Gardasil vaccinations, the authors worked with the National Vaccine Information Center (NVIC) to develop a questionnaire to document symptoms. Families voluntarily completed the questionnaire which was analyzed by the authors and resulted in this report:
While the respondents represent a small sample and the responses have all of the limitations of self-reports, the findings are nevertheless compelling. The data clearly demonstrate consistency in the types and frequency of symptoms experienced following injections of Gardasil that did not exist prior to injection. The symptoms increase in occurrence, number and severity with additional exposure to Gardasil. The graphs and charts reflect a dose-response and temporal relationship. For the 6 deaths reported, there is statistically detectable evidence that the hypothesis that Gardasil is not related to any of them is not tenable. One practical consequence of these findings is that if one experiences certain post-injection symptoms, it may strongly indicate that the inoculation protocol should be aborted.
An article in the Lancet claims that 20 million lives were saved with the use of COVID ‘vaccines’. Where is the evidence for this? How sound is it? Where is the risk benefit analysis? How many lives saved compared to how many excess deaths caused or at least strongly associated with the COVID injections worldwide?
Findings: Based on official reported COVID-19 deaths, we estimated that vaccinations prevented 14·4 million (95% credible interval [Crl] 13·7-15·9) deaths from COVID-19 in 185 countries and territories between Dec 8, 2020, and Dec 8, 2021. This estimate rose to 19·8 million (95% Crl 19·1-20·4) deaths from COVID-19 averted when we used excess deaths as an estimate of the true extent of the pandemic, representing a global reduction of 63% in total deaths (19·8 million of 31·4 million) during the first year of COVID-19 vaccination.
According to a study published Thursday. June 23, 2022 in the journal Lancet Infectious Diseases, nearly 20 million lives were saved by COVID-19 vaccines during their first year, but even more deaths could have been prevented if global targets had been reached. (Pfizer via AP)
A bright red flag is here:
“This work was supported by a Schmidt Science Fellowship in partnership with the Rhodes Trust (OJW), Centre funding from the UK Medical Research Council (all authors), grant funding from WHO (OJW, ABH, PW, and ACG), Gavi, The Vaccine Alliance, and the Bill & Melinda Gates Foundation (JT and ACG), support from the Imperial College Research Fellowship (PW and ABH), and support from the National Institute for Health Research Health Protection Research Unit in Modelling Methodology and Community Jameel (all authors). We thank Sondre Ulvund Solstad from The Economist for developing excess mortality statistics and their help in interpreting these estimates.”
There are clear conflicts of interest in the funding from bodies directly invested in the vaccine industry such as Bill and Melinda Gates Foundation and GAVI.
Imperial College London are the original modellers that grossly over-estimated the expected GOVID deaths leading to policies and practices based on unrealistic fear. They predicted over half a million deaths in the UK and over 2 million deaths in the US. They had a vested interest in balancing the books with a model that produced an outcome with strikingly similar number of ‘lives saved’.
WHO (World Health Organisation) are funded heavily by the Gates Foundation. They are at present lobbying to have global oversight over all future pandemics. Changes to the IHR (International Health Regulations, if successful will give them unprecedented powers including mandating vaccination in all member countries.
Arecent preprint, with the now questionable Medical Journal Lancet, makes the claim that the Covid vaccine introduction in December 2020 actually prevented tens of millions of deaths worldwide.
This paper was submitted by the research group headed by Azra Ghani from the Imperial College of London. Dr. Ghani acts as a consultant for HSBC, GlaxoSmithKline, and the WHO and as with her other Imperial College colleagues, has been pro-lockdown/pro-panic, and pro-vaccine for more than two years.
A single logical fallacy destroys the claims in the piece published on the Lancet. Brownstone (Roger Koops) describes it like this:
“C. Population Susceptibility
The above piece completely ignores the huge gradient in mortality susceptibility in the population. Younger people have had very low infection mortality throughout the past two years. The mathematical models assume the same level of mortality susceptibility across all populations. This assumption we know to be a fallacy and completely negates any of their “models.”
“The mathematical models that have been presented from Imperial College have always been wildly WRONG.”
In other words, the Lancet piece assumes that the young have the same remaining life as the elderly. Ludicrous.
In defence of the unprecedented numbers of reported deaths and serious adverse effects following the Covid injections, the pro-vax “health experts” always retreat to the mythical “20 million lives saved” claim without providing any evidence.
CLICK HERE to view a paper by Makeover, T. et al entitled “Analysis of COVID-19 Vaccination Effectiveness” which was published in May 2023. I quote from this paper:
“By comparing graphs of the intensity of vaccination and the rate of mortality, we see periods of intense vaccination are followed by periods of higher excess mortality. Basic statistical data confirm that COVID-19 vaccines increased the mortality rate” and “it has confirmed that the vaccinated part of the global population has an increased mortality rate of about 14.5% with respect to the non-vaccinated population cohort”.
and here are the numbers from the paper:
Infection fatality ratio (IFR):
The proportion of people infected with SARS-CoV-2 who die from COVID-19.
20 million lives saved? Here are quite recent pre-vaccination IFR data on Covid-19 in the young and working-age population:
“The median [pre-vaccination] IFR was 0.0003% at 0–19 years, 0.002% at 20–29 years, 0.011% at 30–39 years, 0.035% at 40–49 years, 0.123% at 50–59 years, and 0.506% at 60–69 years.”
“At a global level, pre-vaccination IFR may have been as low as 0.03% and 0.07% for 0–59 and 0–69 year old people, respectively.”
‘Age-stratified infection fatality rate of COVID-19 in the non-elderly population’
Professor John Ioannidis (Stanford University) et al.
1 January 2023
Fig. 2. Box plot of infection fatality rate (IFR) estimates across countries per each specified age bin.



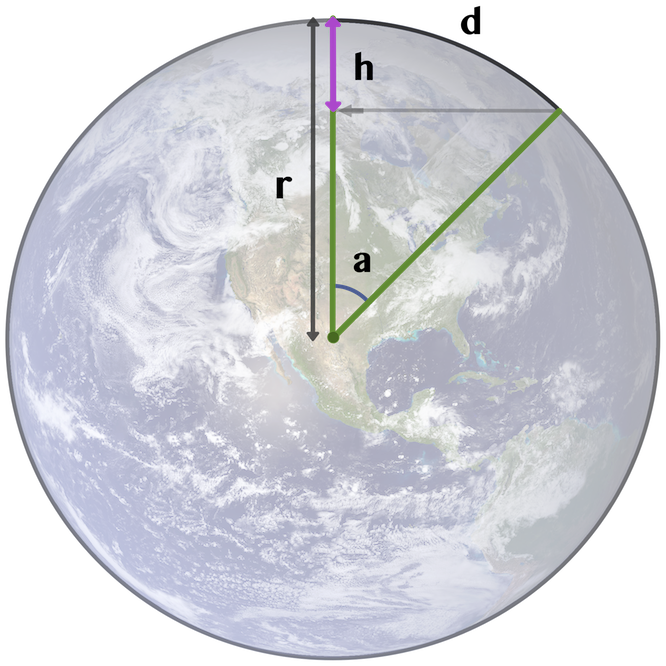
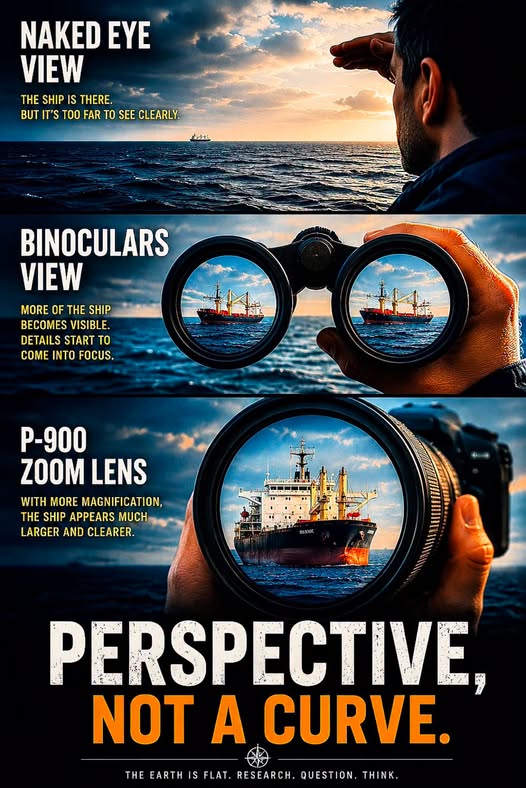
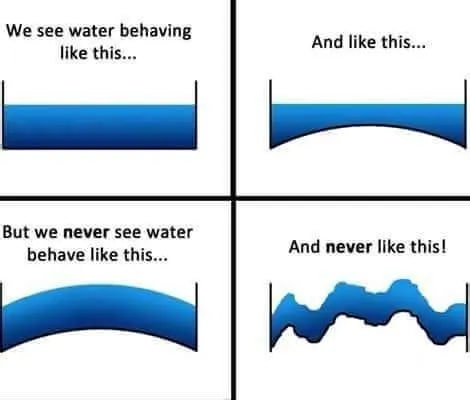

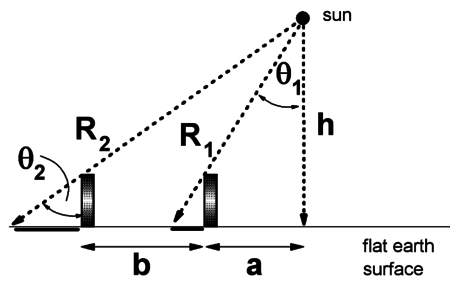
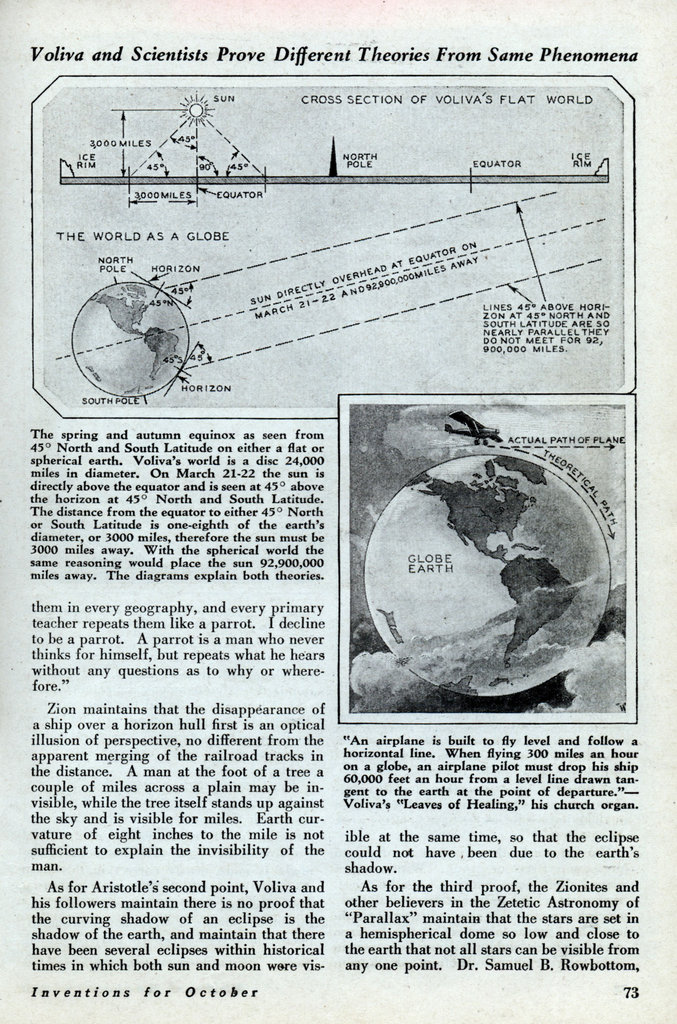

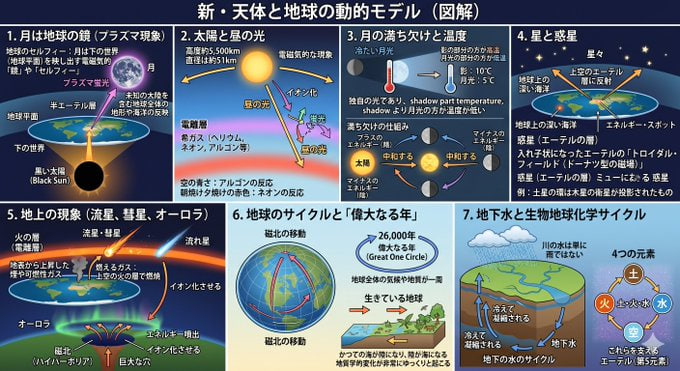










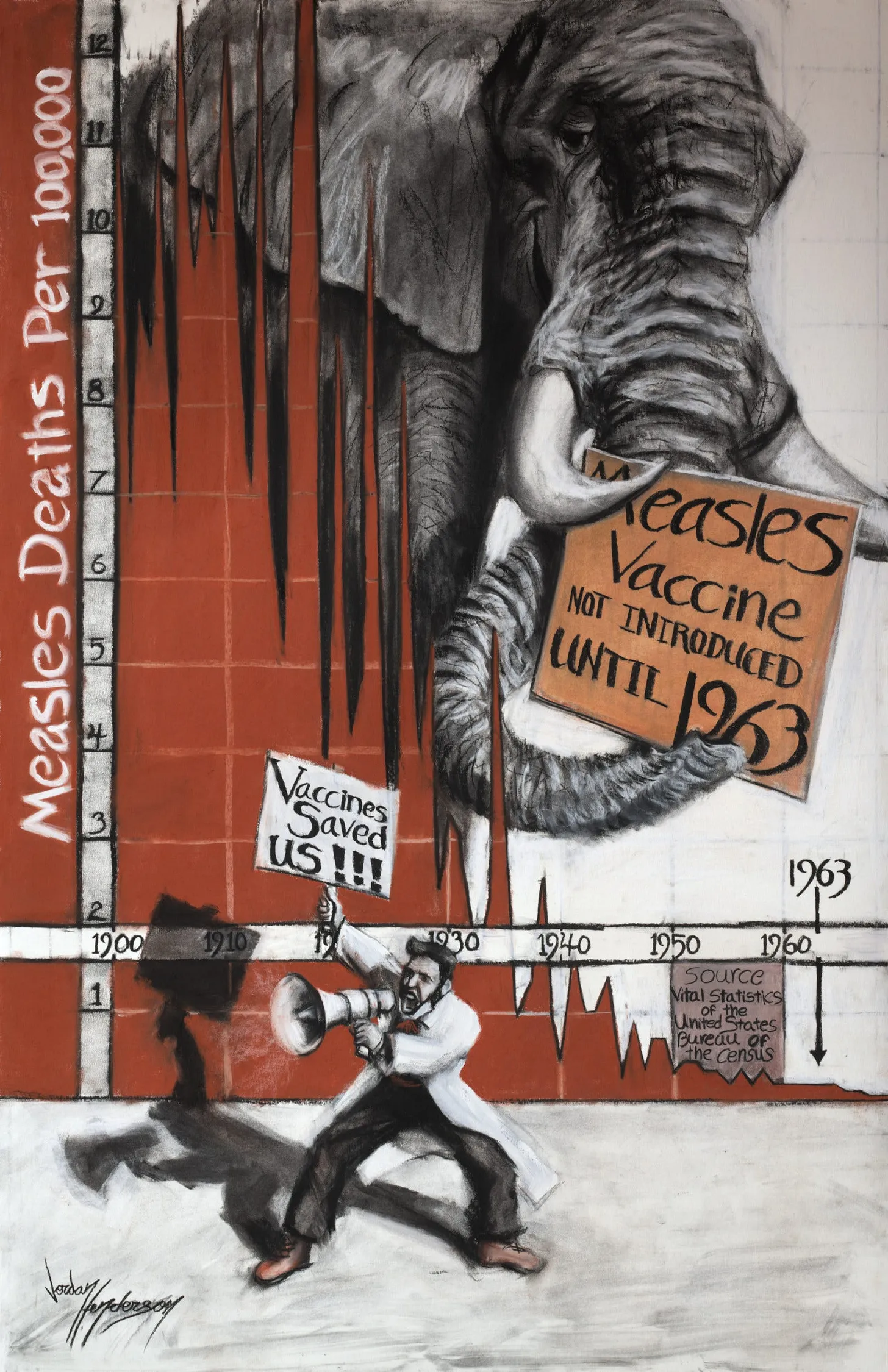

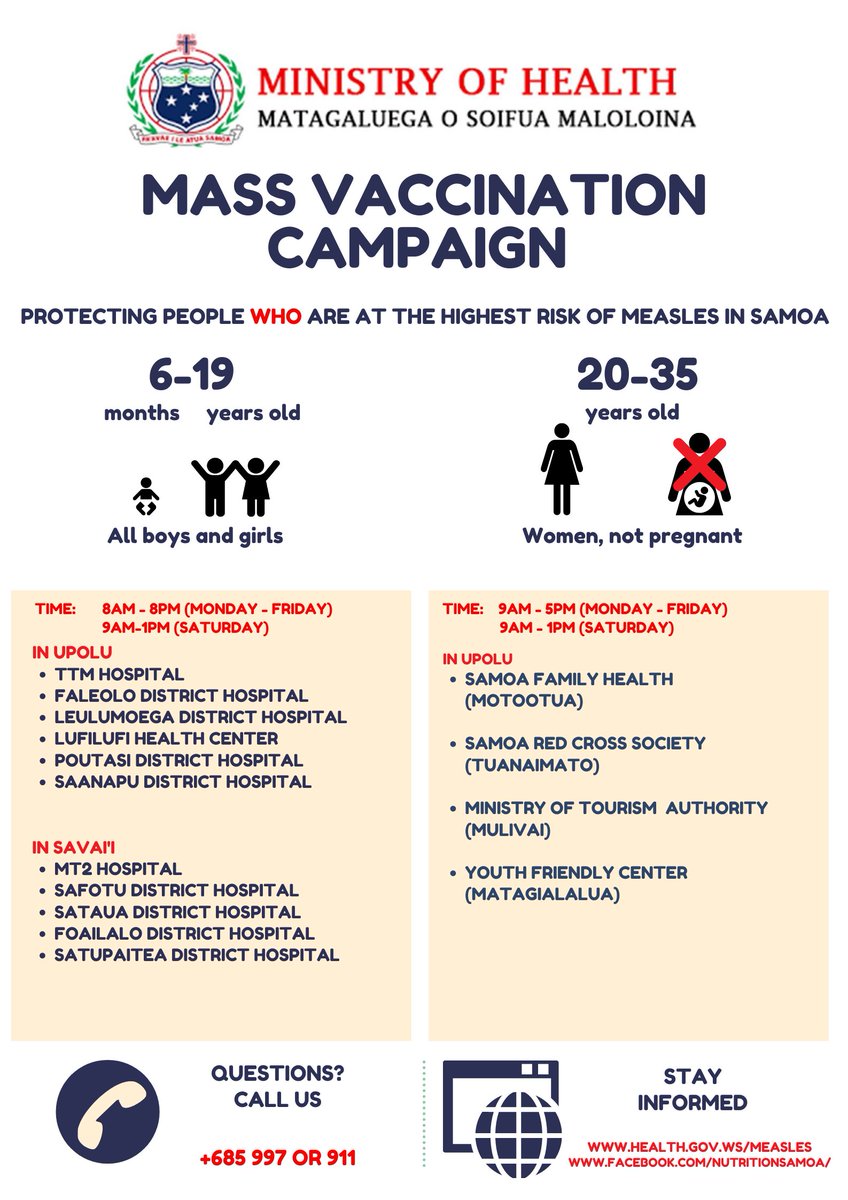










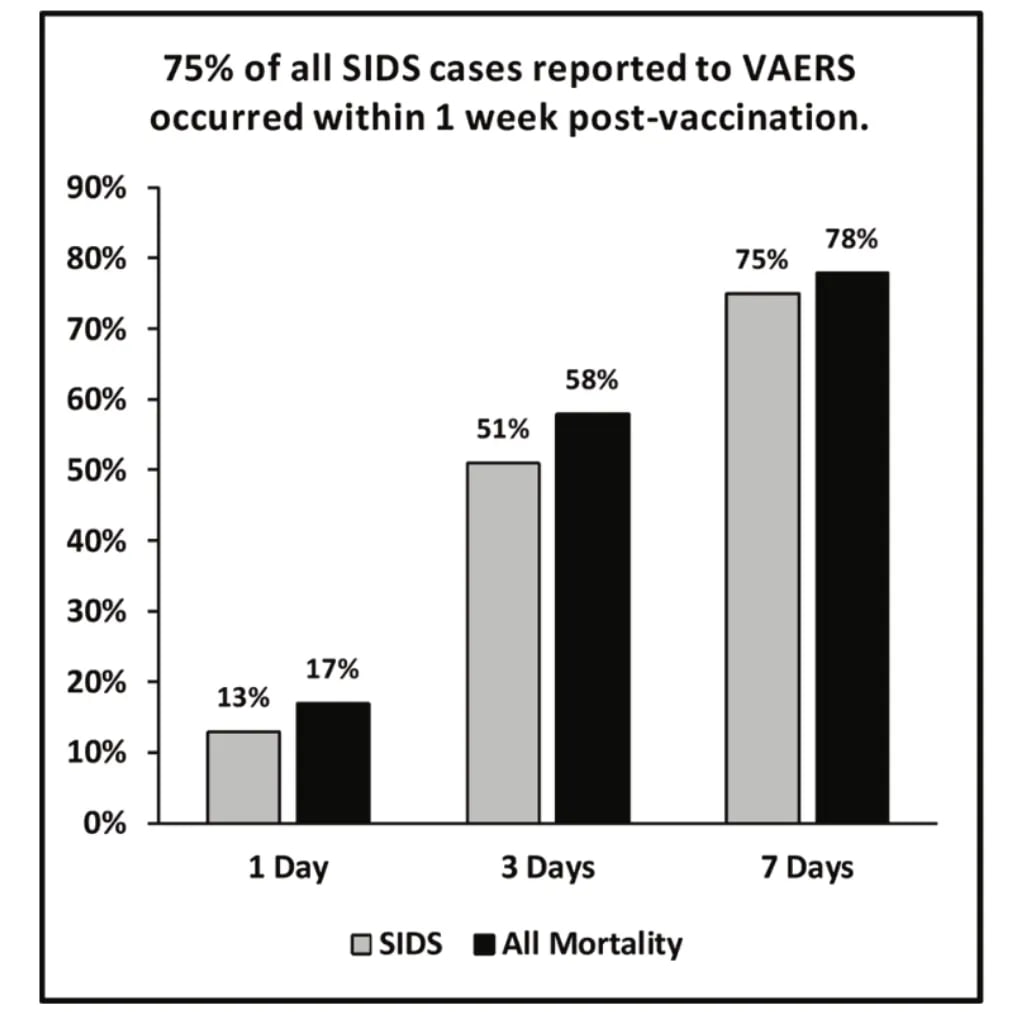

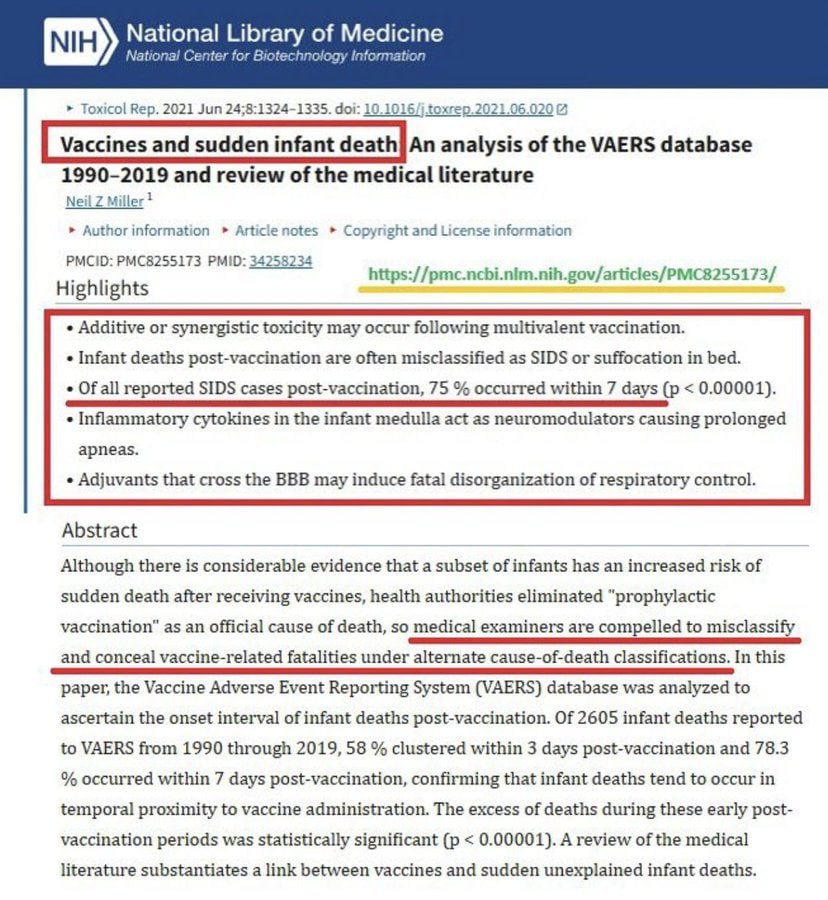
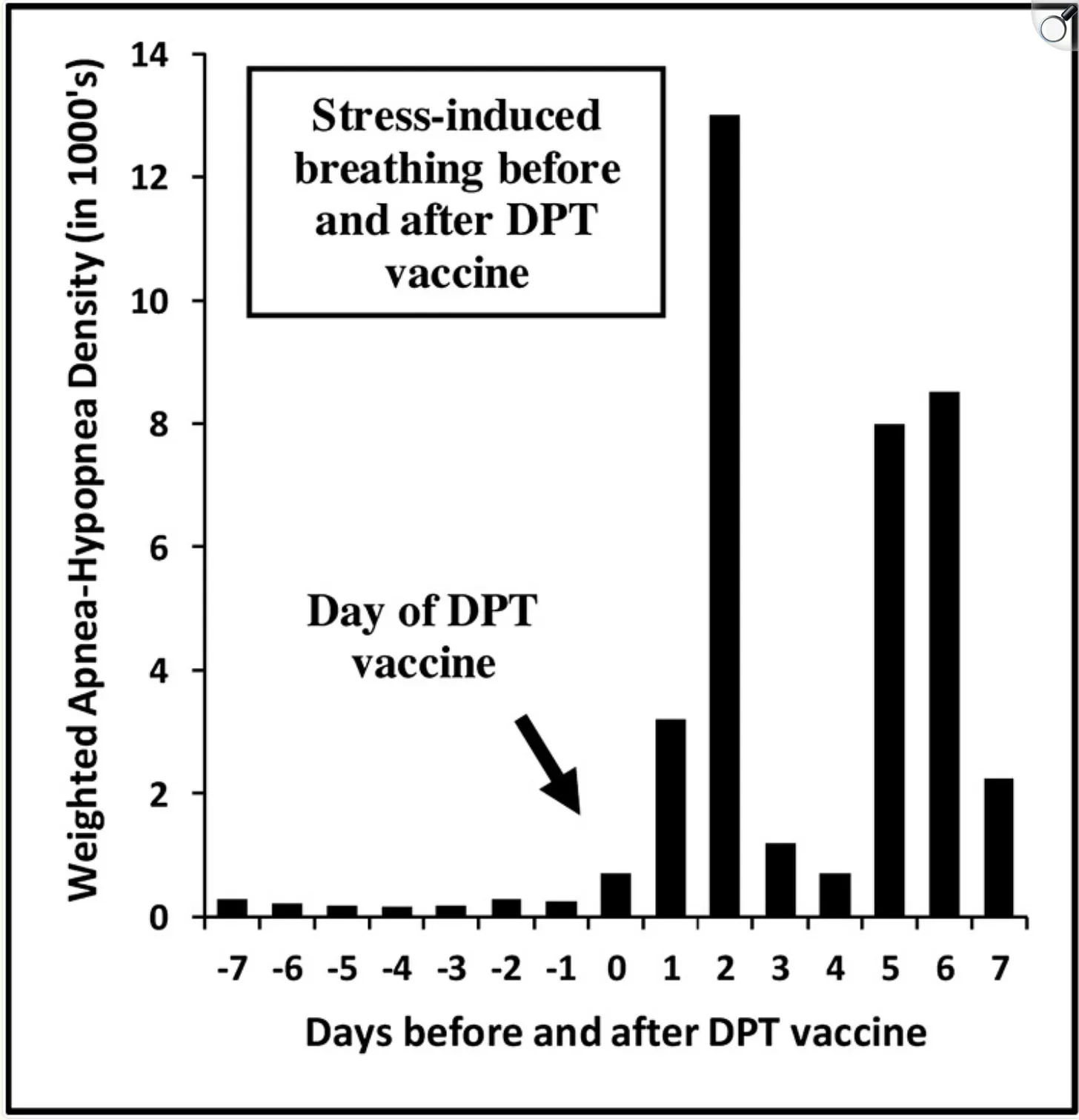
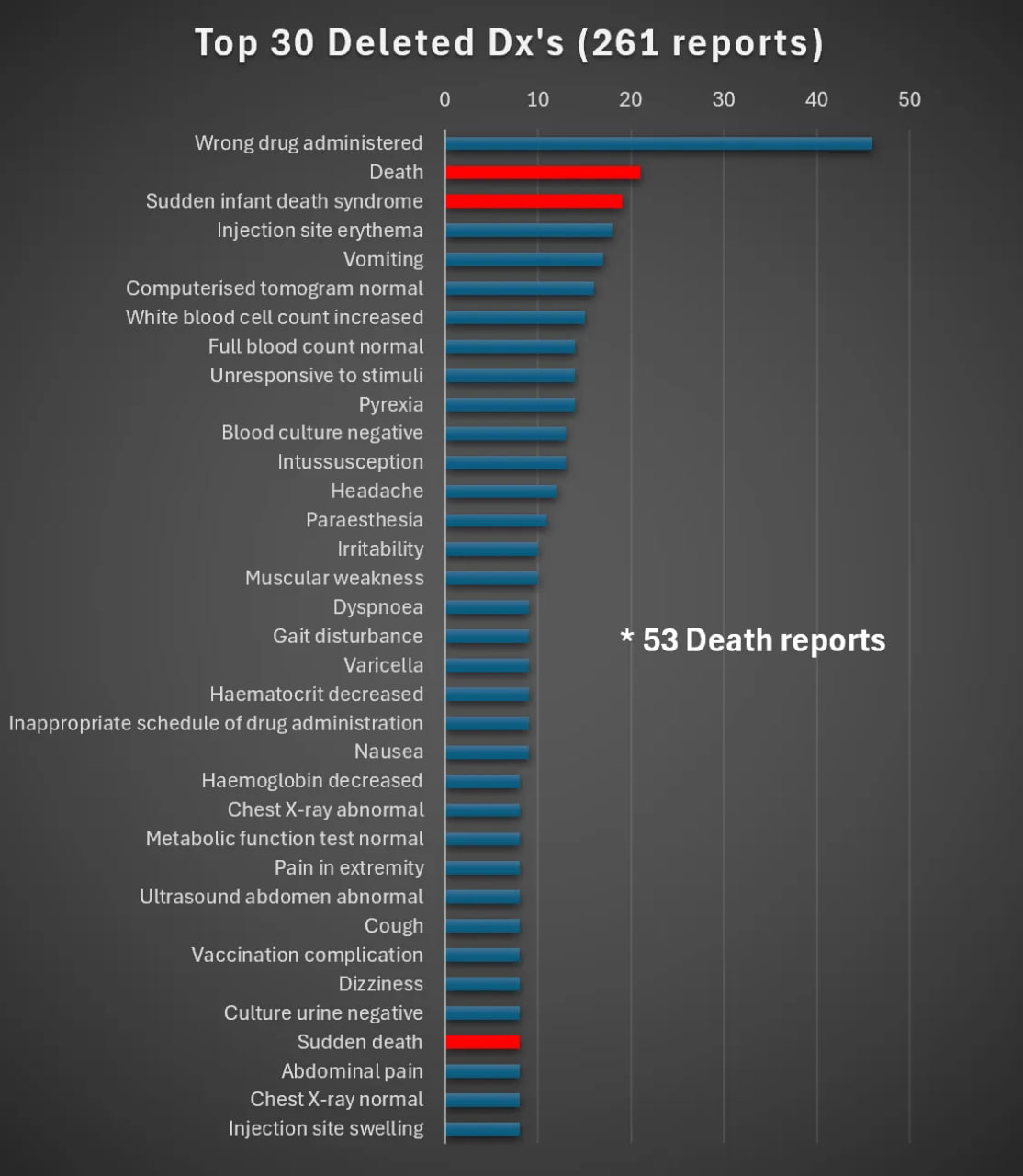


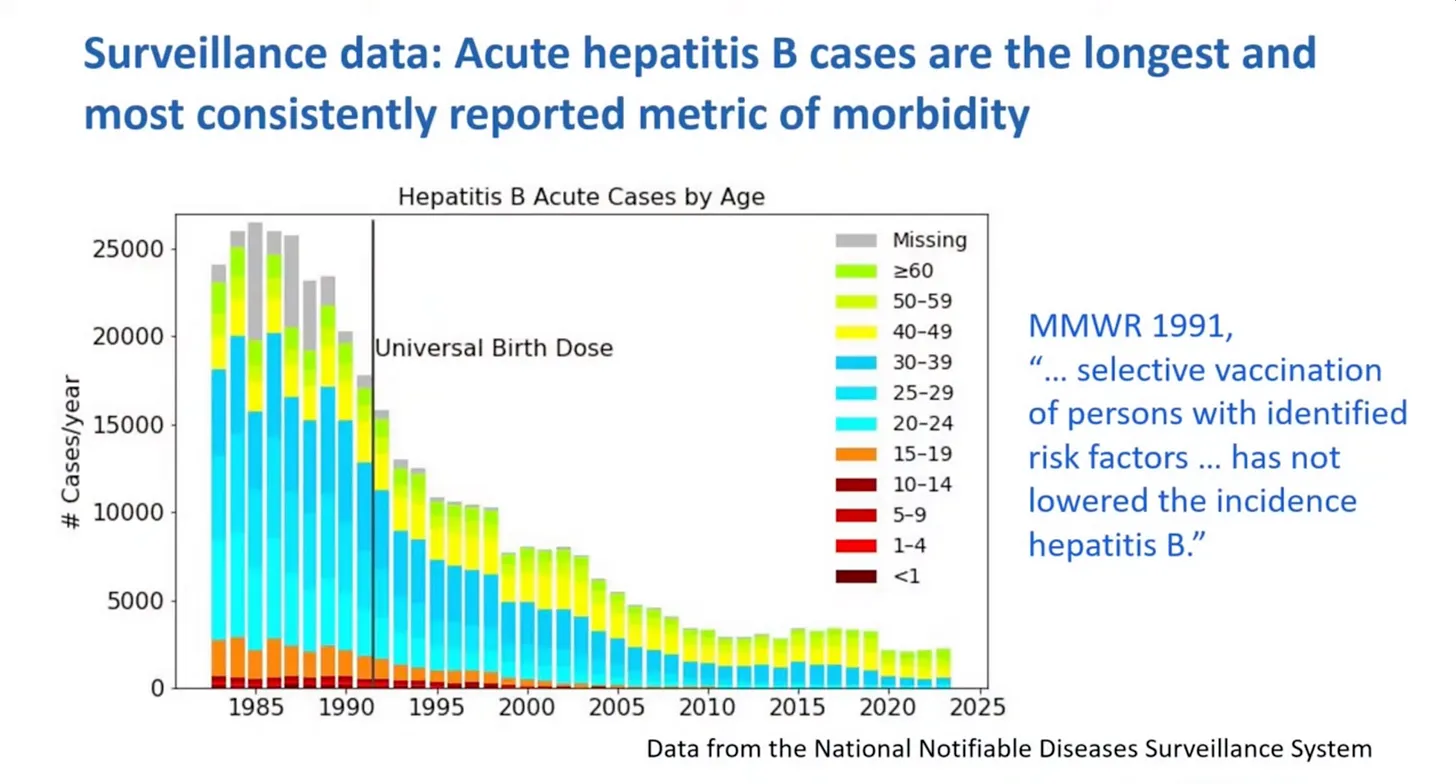
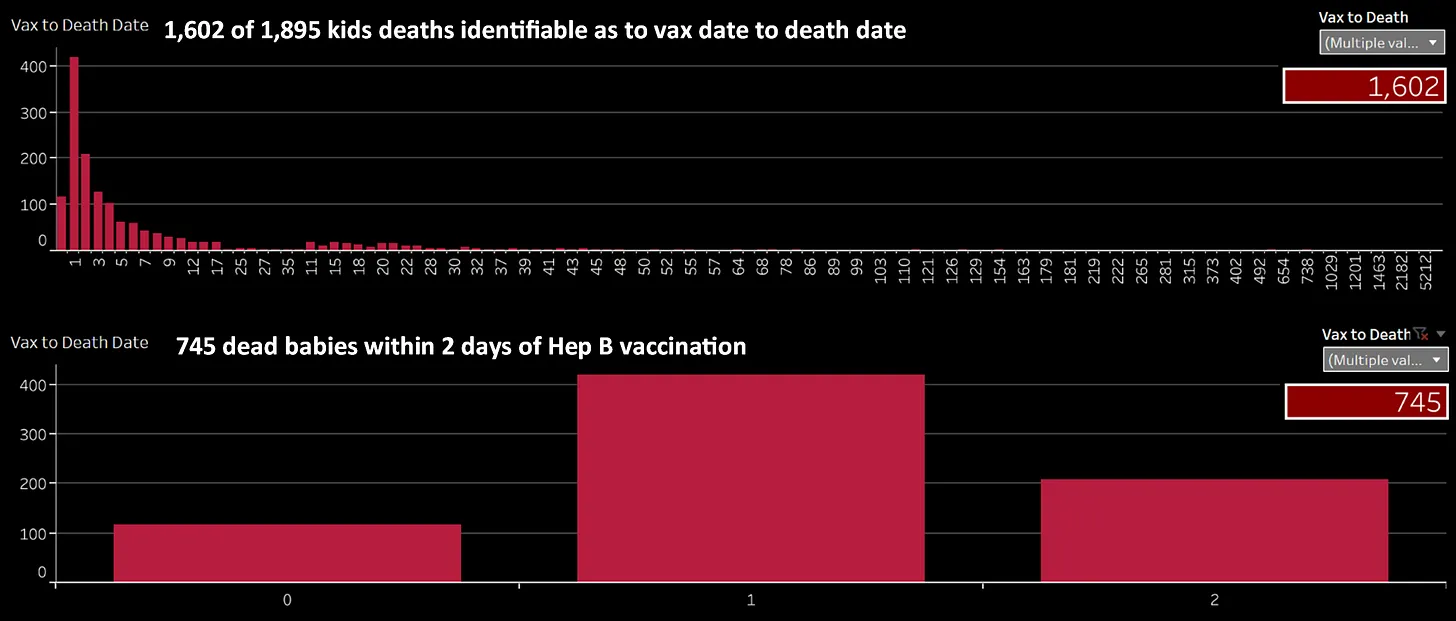



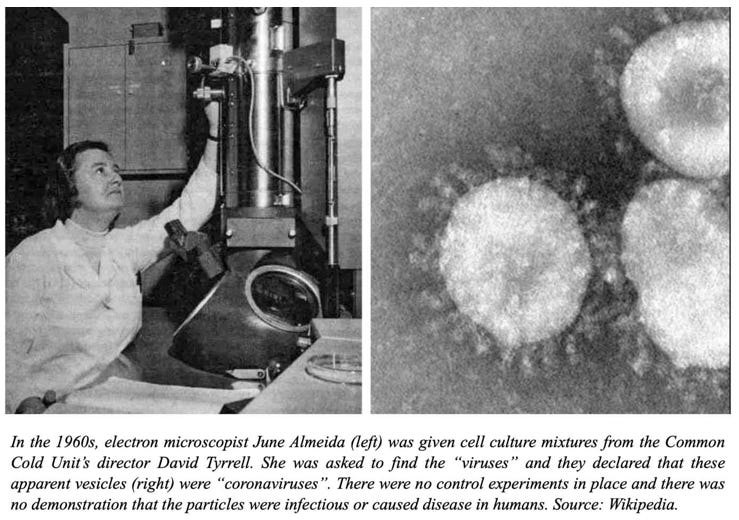
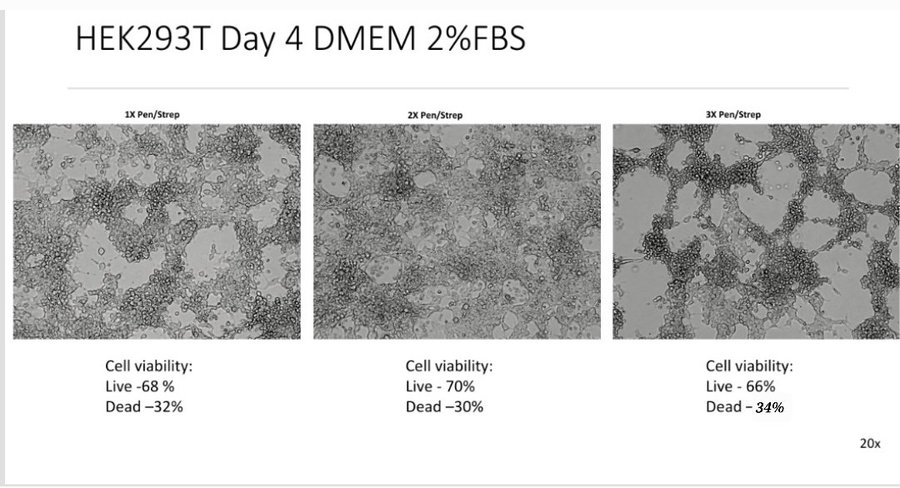
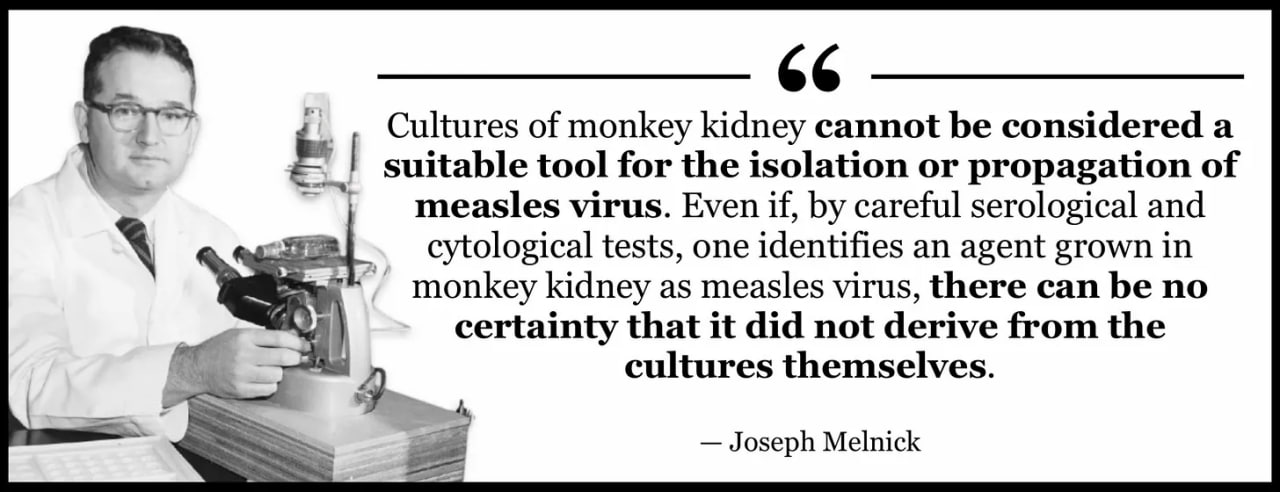

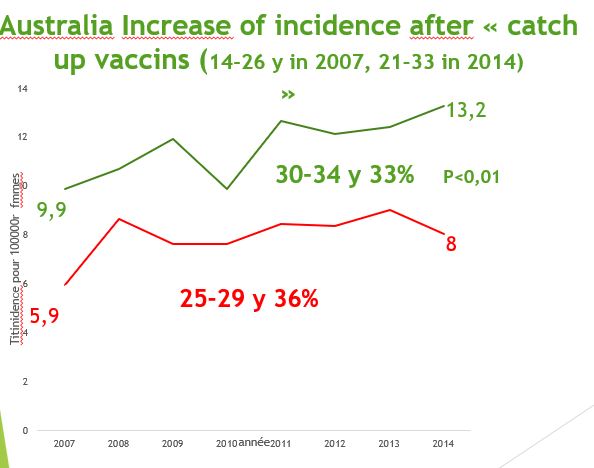



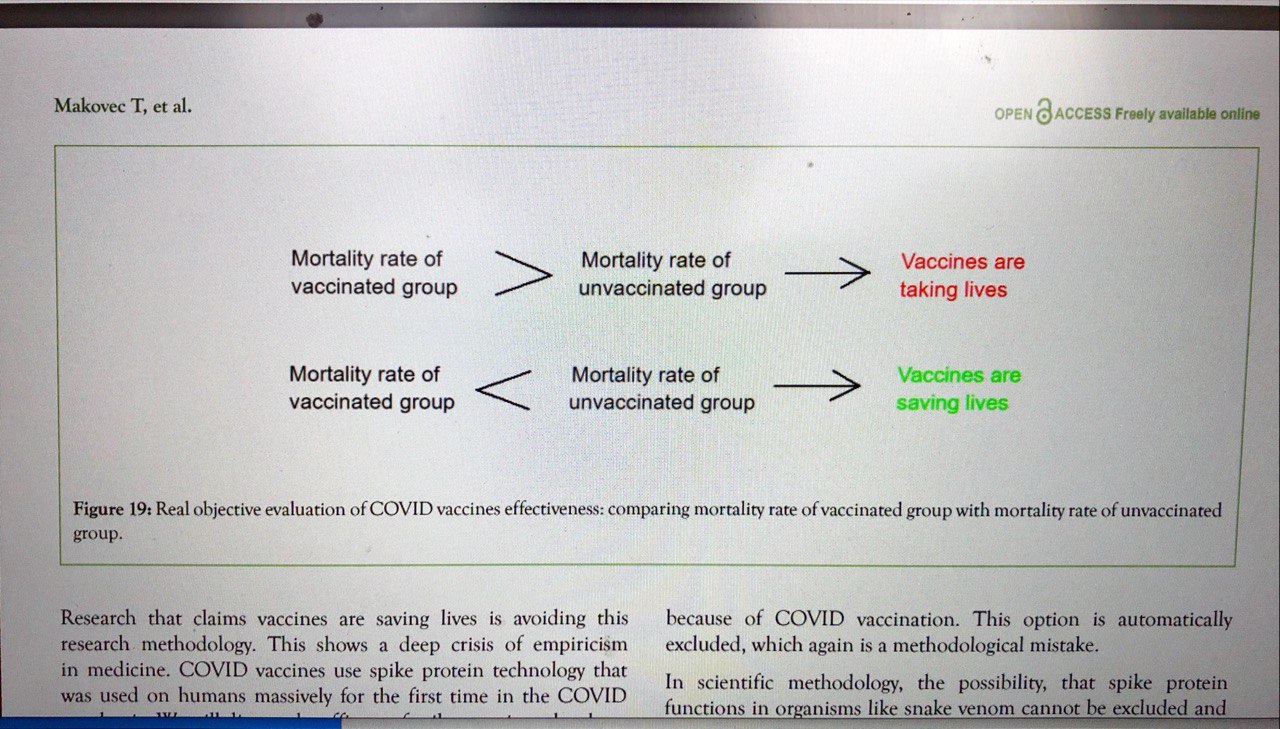
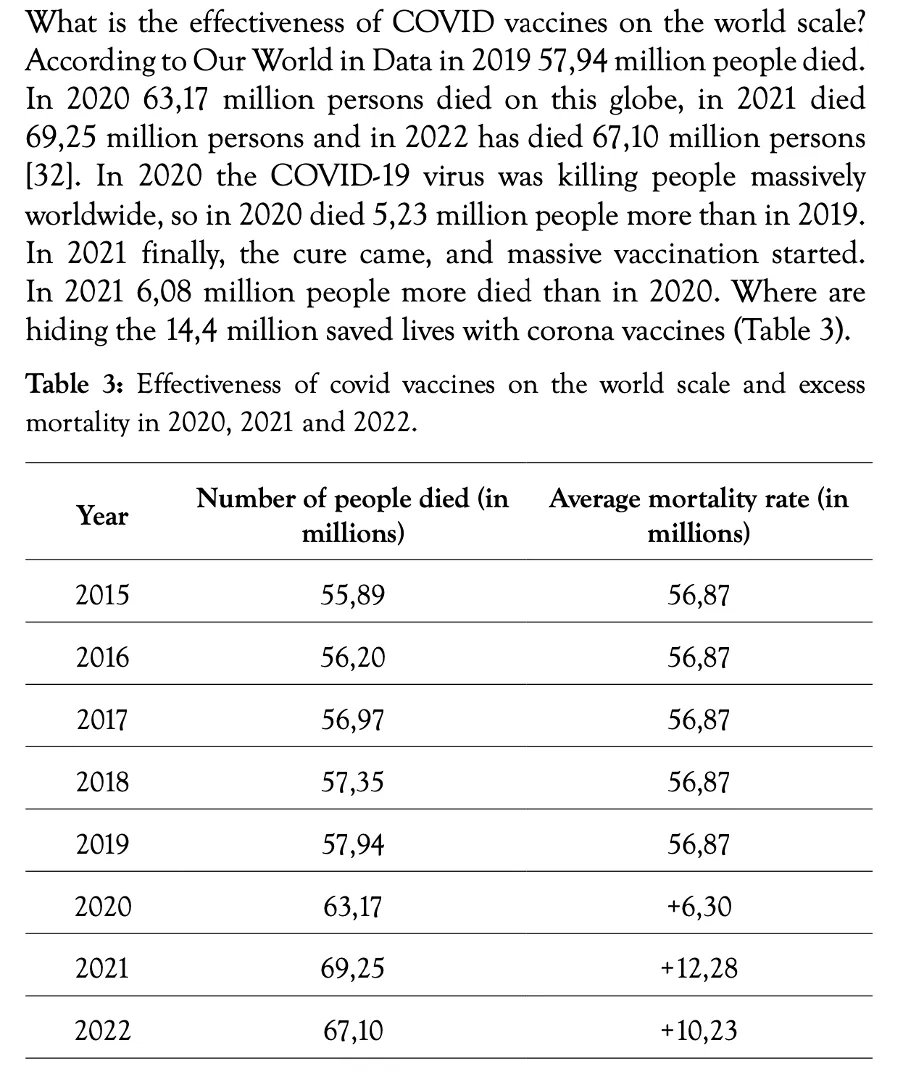
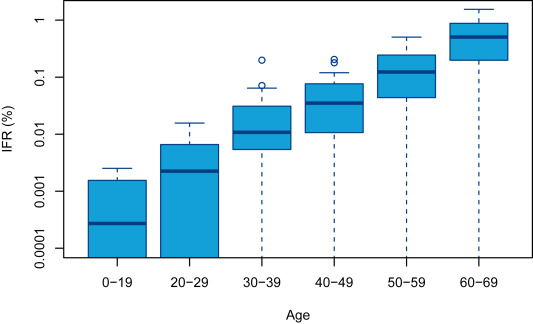
Writes Oz’s Substack
Aug 10: